

Executive Summary
This was the week the group stopped waiting for permission. A Saturday morning lament that the UK has no home-grown frontier model detonated into the busiest day of the week: within two hours members had pledged founding contributions, opened a sign-up document, offered their own GPU hardware, and sketched a plan for a community-owned, open-source UK model with clinical ambitions. A separate aligned group has now been set up to carry the project forward. Around that centrepiece, a consequential news week unfolded: NHS England announced an accelerated AI rollout including AI triage and Microsoft Copilot for 500,000 staff, signalled that EPR-integrated ambient voice technology (AVT) will be favoured in forthcoming guidance, and HSJ revealed the first GMC and NMC complaints over clinicians' use of AI. Meanwhile a member's AVT scribe coded a patient's weight as a temperature, reigniting the data-quality debate, and Scotland's decision to consolidate GP IT onto a legacy system provoked the week's sharpest exchanges about monopoly, interoperability and who really holds suppliers to account.
Activity at a Glance
Week #57 generated 643 messages from 63 contributors, with peak activity on Saturday 4 July (173 messages) as the sovereign model project ignited. Weekend traffic was unusually strong at 42.9% of the total, and Thursday 9 July (116 messages) brought a second surge around imaging referrals and the DCB0129/0160 review. Mornings dominated: the two Saturdays and Thursday each saw sixty-plus messages before noon.
📌 Major Topic Sections
1. "Build it ourselves": the community model and hardware project
The week's defining discussion began with a single wistful message on Saturday morning: "shame we don't have a UK trained frontier model". The group moderator's response, that the group could crowdfund one, "not joking", set off an avalanche. Within minutes a primary care digital policy lead had a sign-up document circulating, and members were declaring themselves in, one observing "we didn't realise the interest in this group. that one message and its exploded with enthusiasm".
The objectives that emerged over roughly 150 messages are worth setting down clearly:
- A community-owned, open-source AI capability for the UK, built from the ground up rather than waiting for government or industry. Members repeatedly framed it as sovereignty in practice: "What a day to start this. 4th July, independence day from US models."
- Start generic, then specialise. The plan is to stand up a general-purpose model on open-source foundations first (GLM 5.2, Qwen, DeepSeek and NVIDIA's conversation models were all discussed as starting points), then build clinical layers on top: a UK speech-to-text solution for medical use and an open-source AVT were named as early targets.
- Community hardware. One digital health GP immediately offered his own training and inference kit (two 96GB GPUs and a 256GB Mac Studio), a GitHub guide to local LLM builds in the £2k-£40k range was shared, and the moderator suggested working out "the minimum hardware build to get something decent" that is also scalable, with a small datacentre as the eventual destination. Pooling under-utilised compute from funded health-tech companies was also floated.
- Community funding. A founding buy-in of around £400 was mooted ("that's 4 months Claude max"), with tiered crowdfunding for smaller contributions, EIS/SEIS-style investment for larger ones, and a charity or CIC structure to hold it. Members flagged the UK sovereign AI fund, UKRI innovation funding and the government's request-for-founders portal as routes to bigger money.
- Routes in for people. Elective, intern and training roles for students and clinicians who want a way into AI work, plus academic partnership to evaluate the results and a federated architecture so the effort can be distributed.
Realism was present too. An NHS clinical AI fellowship lead revealed that a consortium raised over £100m in commitments for exactly this two years ago, only for government to decline its share, and added drily "we also need a few more zeroes". An innovation-focused GP cautioned that training and fine-tuning at scale will cost hundreds of thousands at minimum. The moderator's answer was speed: "MVP approach. If we succeed, push on... in all my career change happens from the ground up." The theme resurfaced the following Saturday with a proposed debate motion that the group has "more than enough talent" to design, build and maintain a home-grown system, "on our own hardware".
A separate aligned group has been set up for those who want to take part. If you would like to know more about the project, its objectives, or how to contribute (skills, hardware, funding or enthusiasm), get in touch with Keith Grimes or Anne Marie Cunningham. (Naming them here is a deliberate, agreed exception to this newsletter's anonymisation policy, so that interested readers have a route in.)
2. The big rollout: AI triage, Copilot for half a million staff, and integration as the baseline
Sunday brought NHS England's announcement of an accelerated AI rollout covering AVT, AI triage and more, with a health-policy analyst noting the named pilot had so far been tested in only a handful of practices and that detail was thin. The item that drew most fire was Microsoft Copilot for more than 500,000 NHS staff, on claimed savings of two admin days per month. A GP educator asked simply for choice: "Will be helpful if we are given a choice rather than be locked into one product." The policy analyst agreed the "one constant in NHS & tech is the market dominance", adding that providers reportedly still have to pay a contribution.
Later in the week a Digital Health story sharpened the direction of travel: NHS England's chief digital, data and technology officer signalled that forthcoming guidance will favour EPR-integrated AVT over standalone tools as part of a £10bn technology package. A clinician and health-tech founder observed from experience that integration is "mostly about usability really", and depends heavily on how willing the EPR partner is. A clinical AI researcher raised a more pointed question: whether pressure to downgrade AVT classification requirements might conveniently suit EPR manufacturers, before adding "tinfoil hat time". The group moderator recalled that AI triage in the NHS is not new, having been embedded in NHS 111 as far back as 2017-2020.
3. Accountability arrives: the first complaints over clinicians' use of AI
Monday's HSJ exclusive landed hard: the GMC received eight complaints against doctors relating to AI use in 2025 and six more in the first half of 2026, with the NMC seeing its first referrals too. Most were closed at triage, but the direction is clear, and a Medical Defence Union adviser quoted in the piece predicted the numbers would "grow over time inevitably". Many complaints appear driven by patients not being told AI was in use, particularly AVT recording consultations.
The group read this alongside the growth of "shadow AI". The article quoted a prominent trust CCIO saying clinicians use unsanctioned AI "because it's incredible" and calling the failure to officially permit such tools "criminal", while the government-commissioned review of AI regulation, due to report this summer, wrestles with the grey areas. An innovation-focused GP predicted most complaints boil down to "I was not informed of the use of AI". The discussion connected directly to Thursday's exchange on the national review of DCB0129/0160: the moderator hoped for greater enforcement, easier acceptance of ISO 14971 in lieu, real support for deployers, and funding so healthcare organisations can actually do the work, while an NHS IT specialist wanted hazard workshops made "central, pivotal" and clinical safety officers "properly recompensed" and skilled in integration, "because that is nearly ALWAYS where the 💩 has gone down".
4. When the code is wrong: a mis-coded weight, a fatal BMI, and the data-quality reckoning
A frontline GP trialling an AVT scribe reported a quietly alarming incident on Monday: at the end of a depression review the patient weighed himself, the transcript correctly captured 77.4kg, and the coded entry recorded a temperature of 77.4°F. He flagged it to the supplier and asked the group: is this a hallucination? He also noted the tool's summaries had changed in style week on week, asking "How do we make sure that 'improvements' don't erode trust in the system".
A patient-safety-focused GP responded with a sobering precedent: a Prevention of Future Deaths report in which an obviously erroneous BMI, never challenged at data entry, contributed to a young man being classed as vulnerable and vaccinated early, with fatal consequence. Members piled in with the state of the art: one GP entered a height of 100cm and weight of 200kg into his clinical system and watched it calculate a BMI of 200 "without a single warning". An integrated care operations lead was blunt: "I really just don't get why clinical systems without challenge guardrails are allowed to continue for as long as they have." The GP who reported the original error revealed he is part of a national group looking at data entry validation, warning it is "not as straightforward to address as might first seem" because there is currently no standard. The thread widened into GP2GP transfer failures, mismatched SNOMED subsets between suppliers, and an innovation-focused GP's verdict from migration work that "it is a miracle we dont have more unfortunate incidents".
5. Gatekeepers and monopolies: imaging referrals, Scotland's GP IT decision, and who holds suppliers to account
Two long, intertwined threads dominated the back half of the week. The first began with an imaging safety and quality lead exploring AI to code patient safety incidents against national radiology taxonomies, and grew into a bracing GP-versus-radiology exchange on referrals: rigid decision-support tools that clinicians route around, IRMER training gaps, requests rejected for missing information that the requester could not attach, and a radiologist member's plea to rediscover the collegiate phone call: "Can we let AI lift some of the admin dross so we can go back to the future of collegiate interaction?" An integrated care operations lead argued referral management likely causes more harm than it saves; a GP and LMC digital lead demonstrated the everyday absurdities, including a trust cross-referencing authorised requestors on a spreadsheet.
The second thread was Scotland. News that Scottish general practice will consolidate onto a single legacy system, while a challenger supplier says it has been refused onboarding to the national framework, provoked genuine anger. A GP partner called it "a crazy backward decision"; a former NHS commissioner in primary care digital described volunteering as a patient for Scotland's app development and being turned away. A digital health consultancy director offered the counter-case: with roughly 450 practices on each of two ageing localised systems, consolidating to one is the lowest-impact option in a market where building NHS-ready products "burns a fortune", and he cautioned against "assumptions from afar". The rejoinders were fierce: "System needs to have at least 3 suppliers to deliver competition", and, from a veteran of the GPSoC era, that the real failure was "the baffling lack of will from the centre to use the various contractual levers they had put in place". The moderator's summary was characteristically practical: has anyone got the DCB0129 and 0160 for the system in question? "We could run CSC-QT across it."
😄 Lighter Moments
The week's funniest thread began with a BBC story about a hospital delivery robot. A practice manager confessed the robot's arm "just has too much of an anal probe look to it for me to be comfortable seeing that trundling down a corridor in my direction", to which a radiologist replied that everyone else had simply thought "Dalek", adding "we don't judge here mate". Warhammer Necrons were also invoked. Niche, but the group delivered.
The World Cup provided a running subplot: post-match outrage over refereeing was soothed with a satirical article claiming FIFA had simply agreed to overturn the USA's loss to Belgium, and one member reported his practice's online triage requests mysteriously dipping the morning after a big match.
Friday became accidental dream-analysis day. An integrated care operations lead described a vividly detailed dream about giving a conference talk titled "The NHS is rubbish at change", complete with agenda. Another member's contribution: "its was a large pig 🐖 pooping 🍬 candy/sweets and then eating it again... dont think it gave any wise ai insight."
And in a moment of perfect newsletter recursion, an innovation-focused GP referred knowingly to a recurring role descriptor in this very publication, prompting the moderator's delighted response: "You've doxxed yourself!"
💬 Quote Wall
"What a day to start this. 4th July, independence day from US models." — AI-enthusiast member
"trying not to use it so that I am content with Opus and Sonnet. A bit like trying not to get into expensive Bordeaux 🍷 so that I don't ruin me for supermarket plonk." — NHS IT specialist, on the last free day of a frontier model
"AI is the most capable intern you've ever had, keen to please, and knows nothing about you or how you work. Onboard them like a new recruit, let them take notes, and debrief when they get things wrong." — Group moderator
"Treat it as a very competent junior assistant with no industry experience." — Integrated care operations lead, on the best AI advice he ever received
"Auscultation doesn't have poor PPV. Humans do. That's a fixable problem." — Clinician and voice-technology founder
"Give me a rule that removes responsibility from judgement." — GP and LMC digital lead, proposing a tutorial topic on clinical decision-making
"It is easy to impose a poor system when you never have to experience the consequences." — GP partner, on commissioner-clinician disconnect
"Monzo want your money. NHS doesn't want any more demand 😉" — Former NHS commissioner, on why bank sign-up is slicker than the NHS App
📎 Journal Watch
Academic Papers and Key Studies
📎 Digital morphine: why AI scribes are symptomatic relief for a broken system – BMJ Digital Health & AI. The paper argues the minutes an AI scribe saves do not create new appointments; they stop the current one spilling into the clinician's evening. Shared as a counterweight to time-saving claims in the week's rollout coverage. Read more
📎 Global workspace theory in LLMs – Anthropic Research. Research suggesting large models may have spontaneously developed an internal "global workspace" (dubbed "J-space"), shared by the moderator alongside his experiments in having models report their internal state during tasks. Read more
📎 Brown professor suspects most of his class used AI to cheat – Inside Higher Ed. Sparked Thursday's education debate: pen-and-paper exams, vivas, and assessment that tests synthesis rather than recall. Read more
📎 BMJ analysis shared during the gatekeeping debate – The BMJ. Shared in the middle of the referral-management discussion as evidence bearing on the costs of demand-management approaches. Read more
Industry and News Articles
📎 Exclusive: first complaints made over clinician use of AI – HSJ. The week's most consequential story: first GMC and NMC complaints over clinician AI use, GMC guidance on responsibility, and the rise of shadow AI. Read more
📎 NHS backs rollout of integrated AVT as part of £10bn tech funding – Digital Health. NHS England signals EPR-integrated AVT will be favoured in guidance over standalone tools. Read more
📎 NHS England to speed up rollout of app AI triage tool to reduce GP demand – Pulse. Prompted the exasperated question: "What is the point of an evidence based intervention!!" Read more
📎 AI triage announcement coverage – BBC News. The story that opened Sunday's rollout discussion; members noted the absence of technical detail. Read more
📎 Beijing is looking at curbing overseas access to China's top AI models – Reuters. Read by members as economic rather than AI warfare, though later analysis shared in the group cast doubt on whether model weights are actually in scope. Read more
📎 Why big AI labs are hiring so many philosophers – The Economist (gift link, time-limited). Shared with the observation that unemployment is currently higher among computer science graduates than philosophy graduates. Read more
📎 Even banks and hyperscalers are now sounding the alarm about the AI bubble – The Register. A cooling counterpoint to the week's enthusiasm. Read more
📎 How OpenAI plans to win over doctors, patients and hospitals – Forbes. Alongside a conference video, taken as clear evidence OpenAI is moving hard into health services; one veteran predicted the classic big-tech pattern of going in hard and retreating two to three years later. Read more
📎 China's dextrous robotic hands – The Guardian. Interactive feature on humanoid robotics progress. Read more
📎 Starbucks bets on AI to replace Microsoft and IBM software – LA Times. Shared with the wry caption that the NHS is surely building its own Office alternative; it fed Saturday's "end of EHRs as we know them" prediction. Read more
📎 Anthropic extends Fable 5 – The New Stack. "Good news for the Fable addicts": the free window on the frontier model was extended mid-week. Read more
📎 China warns Claude Code is leaking user data – TipRanks. A report of claims by Chinese authorities, shared without endorsement amid the week's sovereignty tit-for-tat; the claims themselves are unverified. Read more
Technical Resources and Guidelines
📎 Local LLM build guide – GitHub. "Anyone with 2-40k and looking for something to do with it": the community hardware reference that fed the sovereign model project. Read more
📎 NVIDIA unlocks AI compute at scale – NVIDIA Blog. Shared in support of the pooled-compute funding idea. Read more
📎 GPT-5.6 benchmarks – Simon Willison. For those asking about the newest OpenAI release. Read more
📎 Adequate completion of radiology request forms audit template – Royal College of Radiologists. Surfaced during the hunt for imaging-request guidance suitable for conversion into an AI skill; described by one frontier model, memorably, as "a sound, if elderly, audit recipe". Read more
📎 MHRA Yellow Card for software, apps and AI – MHRA. Proposed as the route to surface systems that fail to meet standards. Read more
📎 UK data sovereignty podcast episode – Pocket Casts. Recommended listening for the sovereignty-minded. Read more
📎 Member-built GP data explorer – GitHub Pages. A member's natural-language question interface over GP access and continuity datasets, offered to the group for road-testing ("try and break it"), with a practice-level companion tool. Read more Read more
Policy Documents and Official Reports
📎 NHS accelerates artificial intelligence rollout – NHS England. The official press release behind the week's rollout coverage. Read more
📎 National review of clinical risk management standards (DCB0129/0160) – NHS England Engage. The open consultation that prompted Thursday's discussion of what strengthened standards should look like. Read more
📎 Prevention of Future Deaths report: Alexander Reid – Judiciary UK. The erroneous-BMI case that anchored the data-quality discussion. Read more
📎 UKRI innovation funding portal – Apply for Innovation Funding. Flagged as a funding route for the community model project, alongside the government sovereign AI founders call. Read more Read more
🔭 Looking Ahead
The community model project moves to its next phase: collating ideas, a first organising meeting, and structure decisions (charity, CIC or something else). Get in touch with Keith Grimes or Anne Marie Cunningham to join the aligned group. The DCB0129/0160 consultation remains open and the group is clearly minded to respond. The government-commissioned review of AI regulation is due to report this summer, and the first complaints data suggests professional regulators will feature in future issues. A BMJ survey on the state of digital health integration across Europe is gathering group perspectives, and members await the promised detail behind NHS England's AI rollout announcement.
🧬 Group Personality Snapshot
This week showed the group at full range: capable of turning a Saturday-morning grumble into a funded-in-principle sovereign AI project before lunch, and equally capable of spending Wednesday evening arguing about whether an ultrasound requires ionising radiation regulations. It is a community where a radiologist and several GPs can trade genuinely pointed criticism about referral gatekeeping and end with drum-roll emojis; where a member cheerfully identifies himself by his own anonymised newsletter descriptor; and where the response to national policy frustration is not resignation but a Google Doc, a hardware inventory and a name-brainstorm of dubious acronyms. The prevailing mood: impatient, practical, and increasingly convinced that if the future is going to be built, it may as well be built here.
APPENDIX A: Detailed Activity Analytics 📊
📬 Total Messages: 643
📈 Peak Day: Saturday 4 July (173 messages)
🔥 Most Active Period: Saturday 4 July, 09:00-12:00
💬 Average/Active Day: 80 messages
🏖️ Weekend Activity: 42.9% (276/643)
💼 Weekday Activity: 57.1% (367/643)
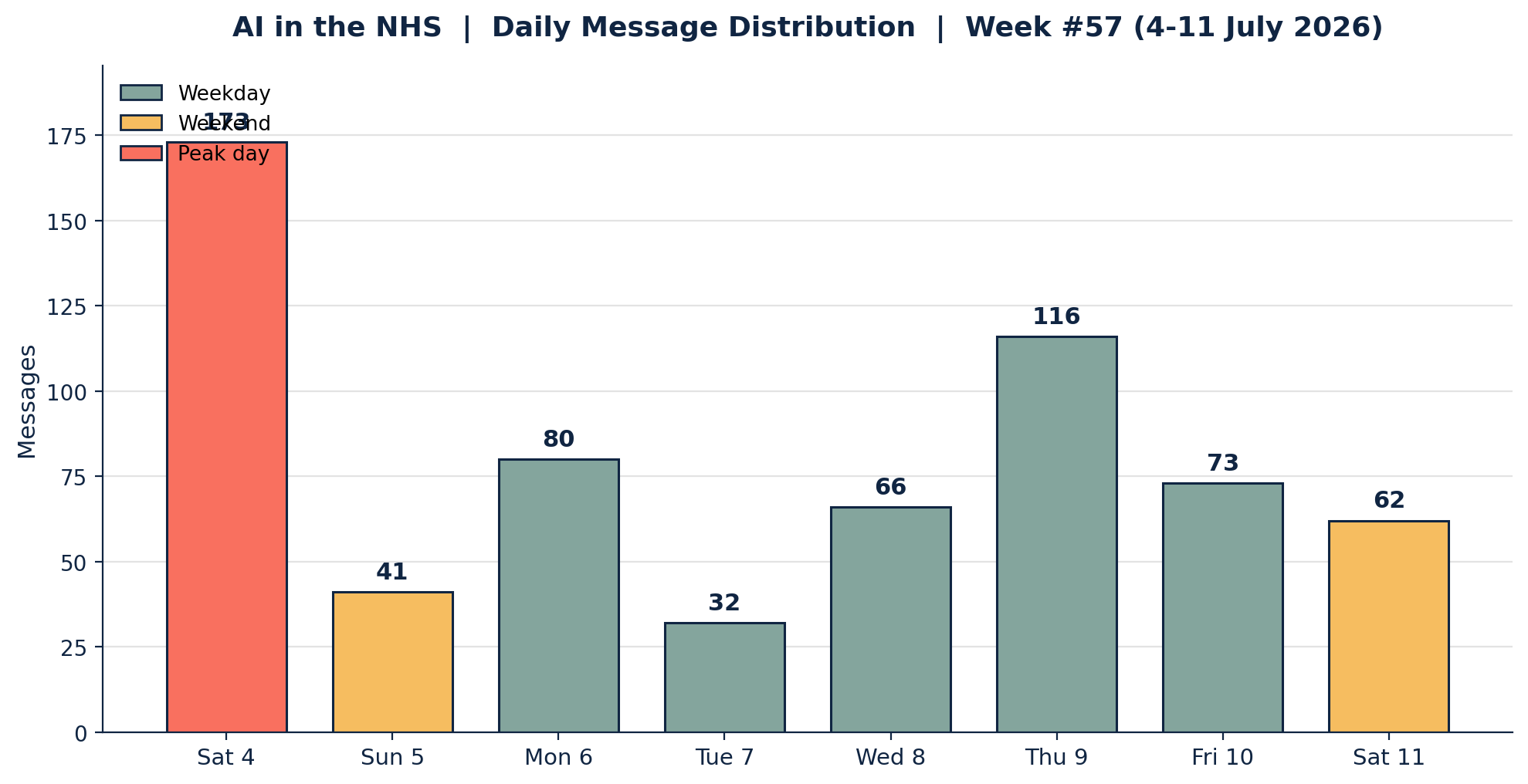
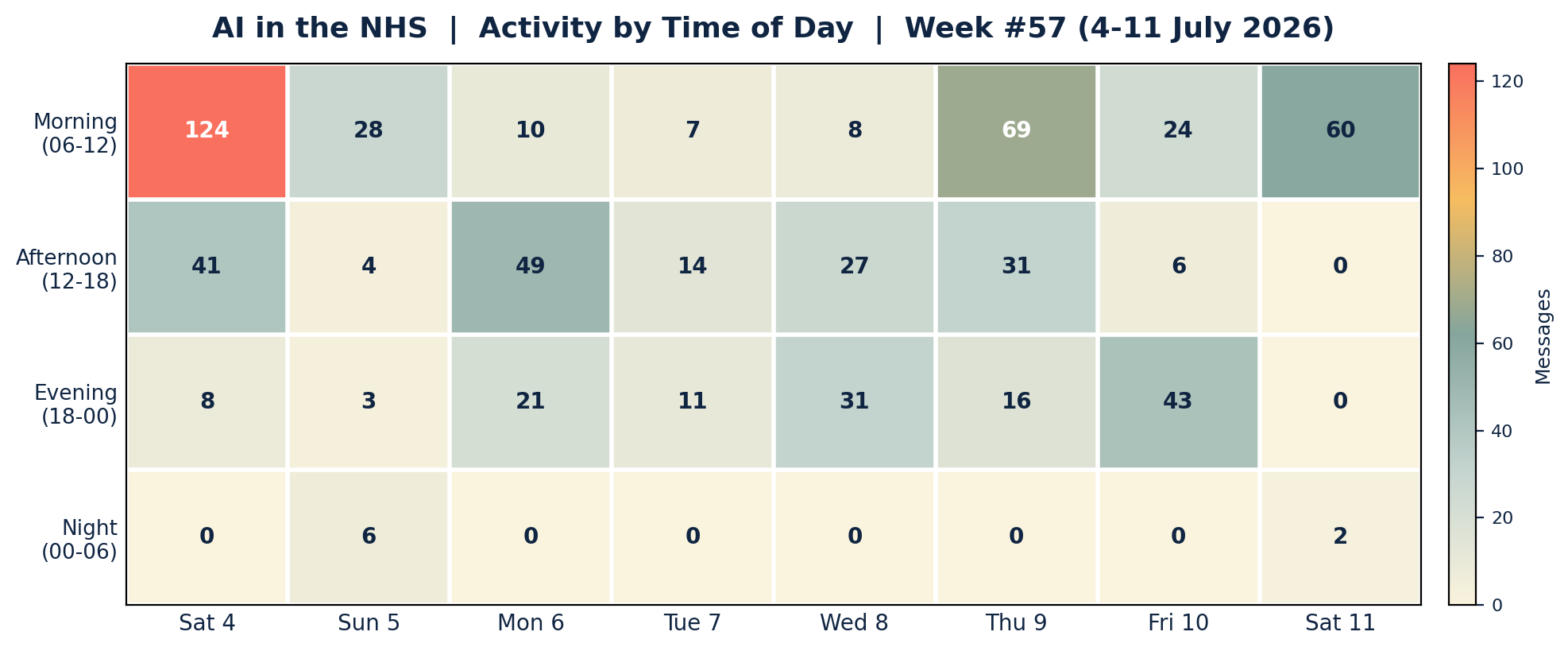
Insights: The week inverted the usual weekday-dominant pattern: 42.9% of traffic fell on the three weekend days, driven almost entirely by the sovereign model eruption on the morning of Saturday 4 July (124 messages before noon, the densest three-hour window in recent issues). Thursday produced the strongest weekday showing, with the imaging referral debate running from breakfast to midnight. Note that the coverage window runs 09:00 Saturday to 09:00 Saturday, so the two Saturdays are each partial days; that the truncated opening Saturday still logged 173 messages underlines how explosive the project launch was. Evening activity clustered late in the week, with Friday's supplier-monopoly exchanges running past 23:00.
APPENDIX B: Enhanced Statistics
Unique Contributors: 63 group members posted at least one message this week. The 10 most active below account for 419 of the 643 messages (65.2%), with a long tail of occasional and one-off contributors making up the rest.
Top 10 Contributors (Role Descriptors Only):
1. Digital Health & Clinical AI Specialist (Group Moderator): 125 messages
2. GP and LMC Digital Lead: 50 messages
3. Innovation-Focused GP: 46 messages
4. Radiologist and Clinical Governance Advocate: 38 messages
5. AI-Enthusiast Group Member: 36 messages
6. Integrated Care Operations Lead: 35 messages
7. Digital Health Contributor: 27 messages
8. Primary Care Digital Policy Lead: 22 messages
9. Veteran Health Informatician and Medical Appraiser: 21 messages
10. NHS IT Specialist: 19 messages
Hottest Debate Topics:
1. 🔥🔥🔥 The community-built sovereign UK model: funding, hardware, structure (roughly 160 messages across 3 days)
2. 🔥🔥🔥 Imaging referrals, gatekeeping and incident coding (roughly 120 messages across 2 days)
3. 🔥🔥 Scotland's GP IT decision, monopoly and interoperability (roughly 70 messages across 2 days)
4. 🔥🔥 Data quality: AVT coding errors, BMI validation and GP2GP (roughly 50 messages, 1 day)
5. 🔥 NHS AI rollout: triage, Copilot and integrated AVT (roughly 40 messages across 3 days)
6. 🔥 AI, education and the future of reflection and assessment (roughly 30 messages across 3 days)
Discussion Quality Metrics:
• Evidence-Based vs Opinion Ratio: roughly 30% of substantive messages referenced articles, official documents, papers or first-hand data
• External Resource Sharing: 50+ unique links shared across the period
• Constructive Challenge Rate: high this week; every major thread featured direct, civil disagreement (GP vs radiologist on referrals, supplier vs consultant on Scotland, enthusiasm vs realism on the sovereign model)
• Average Thread Depth: the two longest threads each sustained engagement across a full day or more
Cross-Expertise Engagement:
• At least 15 distinct professional backgrounds contributed: GPs (partners, trainers, LMC and federation roles), a radiologist, a hospital consultant, practice managers, NHS IT and informatics specialists, an imaging quality lead, EPR and online-consultation suppliers, health-policy analysts, a former commissioner, health-tech founders, academics and educators
• Most cross-disciplinary discussion: the imaging referral thread, which brought GPs, a radiologist, informaticians, a Welsh national systems specialist and an imaging safety lead into a single sustained exchange
• Notable knowledge transfer: Welsh order-comms design (eGFR surfacing at request time) offered as a working answer to England's ICE frustrations; supplier-side detail on GPSoC contractual levers; radiology-side explanation of IRMER requestor lists
APPENDIX C: Daily Theme Summary
Saturday, 4 July 2026
Primary Theme: The community sovereign model project ignites Key Discussion: From "shame we don't have a UK trained frontier model" to a sign-up document, founding pledges, hardware offers and funding routes inside two hours. Objectives crystallised around an open-source foundation, clinical specialisation (UK medical STT, open-source AVT), community hardware and a charity/CIC structure. Secondary Discussions: LLMs, adverts and pharma compliance; health literacy and whether AI answers erode understanding of "why"; an NHS shout-out at a music festival. Notable: Peak day of the week (173 messages despite the 09:00 window start). A precedent consortium that raised £100m+ in commitments was revealed.
Sunday, 5 July 2026
Primary Theme: NHS England's AI rollout announcement Key Discussion: AI triage pilots, Copilot for 500,000 staff and vendor lock-in worries; thin technical detail noted. Babylon's 111 triage history recalled. Secondary Discussions: Whether AVT erodes trainee thinking; "AI as competent junior assistant" framing; philosophers in AI labs; the "digital morphine" paper on scribes. Notable: First connections drawn between the rollout and the previous day's sovereignty argument.
Monday, 6 July 2026
Primary Theme: Accountability and data quality Key Discussion: HSJ's exclusive on the first GMC/NMC complaints over clinician AI use; then the AVT scribe that coded 77.4kg as 77.4°F, the erroneous-BMI Prevention of Future Deaths report, and the absence of data-entry validation standards. Secondary Discussions: GP2GP and SNOMED subset failures; a successful EPR migration go-live; last free day of a frontier model; LLM "global workspace" research. Notable: Issue #56 of this newsletter published mid-discussion.
Tuesday, 7 July 2026
Primary Theme: Robots, China and OpenAI's health ambitions Key Discussion: A hospital delivery robot's questionable aesthetics; Beijing reportedly weighing limits on overseas access to Chinese models, read as economic strategy; OpenAI's health services ambitions dissected. Secondary Discussions: A member's AI incident-coding project introduced; a member-built GP data explorer shared; BMJ digital health survey. Notable: Quietest day of the week (32 messages).
Wednesday, 8 July 2026
Primary Theme: Incident coding, PSIRF and imaging governance Key Discussion: Using AI to code patient safety incidents against national radiology taxonomies; PSIRF's limits for specialty-specific pathways; reporting friction as the real barrier ("most... can't hide a dead body, but rarely can be arsed to report"). Secondary Discussions: IRMER and non-medical referrers; World Cup refereeing outrage; auscultation's diagnostic value and computerised respiratory sound analysis. Notable: The auscultation exchange ended with a voice-technology founder offered a clinical test site.
Thursday, 9 July 2026
Primary Theme: Imaging referrals and the gatekeeping debate Key Discussion: Rigid decision-support tools, rejected referrals, spreadsheet-based requestor lists and the case for AI lifting admin so collegiate conversation can return. Referral management's harms argued forcefully. Secondary Discussions: The DCB0129/0160 national review and what better standards would look like; AI and education (Brown cheating story, viva assessment, an AI-permitted masters module); NHS England's integrated-AVT guidance signal. Notable: Second-busiest day (116 messages), running from 07:39 to 23:03.
Friday, 10 July 2026
Primary Theme: Workforce, appraisal and the escape from the NHS Key Discussion: An appraiser's observation that young doctors are "escaping" a "toxic culture"; portfolio careers; the cost and value of independent appraisal. Secondary Discussions: Vivid work dreams; AI-generated message "slop"; a consultation-feedback training tool pitched; Scotland's GP IT single-supplier decision breaking late evening. Notable: The Scotland thread ran past 23:00 and carried into Saturday.
Saturday, 11 July 2026 (to 09:00)
Primary Theme: Monopoly, commissioning and who holds suppliers to account Key Discussion: Scotland continued: framework refusals, GPSoC history, the NHS App vs the market, ICBs reportedly blocking practice EPR moves, and the economies-of-scale counter-argument. "Conformity to standards - not to products or companies." Secondary Discussions: The end of EHRs as we know them; a debate motion on the group's capacity to build its own system "on our own hardware"; MHRA Yellow Card for software. Notable: The sovereignty theme closed the week exactly where it opened it.
AI in the NHS Weekly Newsletter is produced by Curistica Ltd for members of the AI in the NHS WhatsApp community. All contributors are anonymised. Views expressed are those of individual community members and do not represent any organisation.



