Executive Summary
This week the group put ambient voice technology under a microscope and did not entirely like what it saw. A quality claim relayed from a national congress, that AVT improves ambulance notes and saves ten to fifteen per cent of clinician time, triggered a hard-headed thread about who actually benefits, whether the time saved buys "cognitive headroom" or simply more patients, and where the independent, conflict-free evidence has got to. A newly-joined clinician and voice-technology founder then took the group deep into the physics of capture, arguing that the source signal is the whole asset and that a cheap microphone, a lossy codec and a cloud hop quietly destroy the fidelity a model needs, while frontline members swapped confabulations from their own scribes ("hydroxychloroquine heard in a conversation about eye drops"). The practical consensus was old and unglamorous: check the microphone first, define your evaluation, and never assume a scribe that never hallucinates is the safe one.
Running underneath was a sharper argument about the rules. An HSJ exclusive that regulators are "poised to strip back AI rules" split the group between those who read it as bold competitive positioning and those who called it deregulating patient safety, "about as daft as deregulating motorcycle helmets because they get too stuffy on hot days." The moderator's repeated answer was to stop waiting for the regulatory weather and take control of your own governance, with DCB0129/0160 as the pragmatic route in, timely given the national review consultation on those very standards opened the same week. The counter-example arrived on Wednesday when a UK ambient voice tool became the first to reach UKCA Class IIa certification, celebrated as proof that doing it properly is possible. Add an open-source surge (even Palantir was seen endorsing open weights), a genuinely busy week from Anthropic (Sonnet 5, Claude Science and Fable), a bruising debate about outsourcing trainee reflection to AI, a return to the statins-versus-exercise value question, and a Palantir and Federated Data Platform trust saga that ended the week with a watchdog investigation, and you have 489 messages. Here are the threads that shaped them.
Activity at a Glance
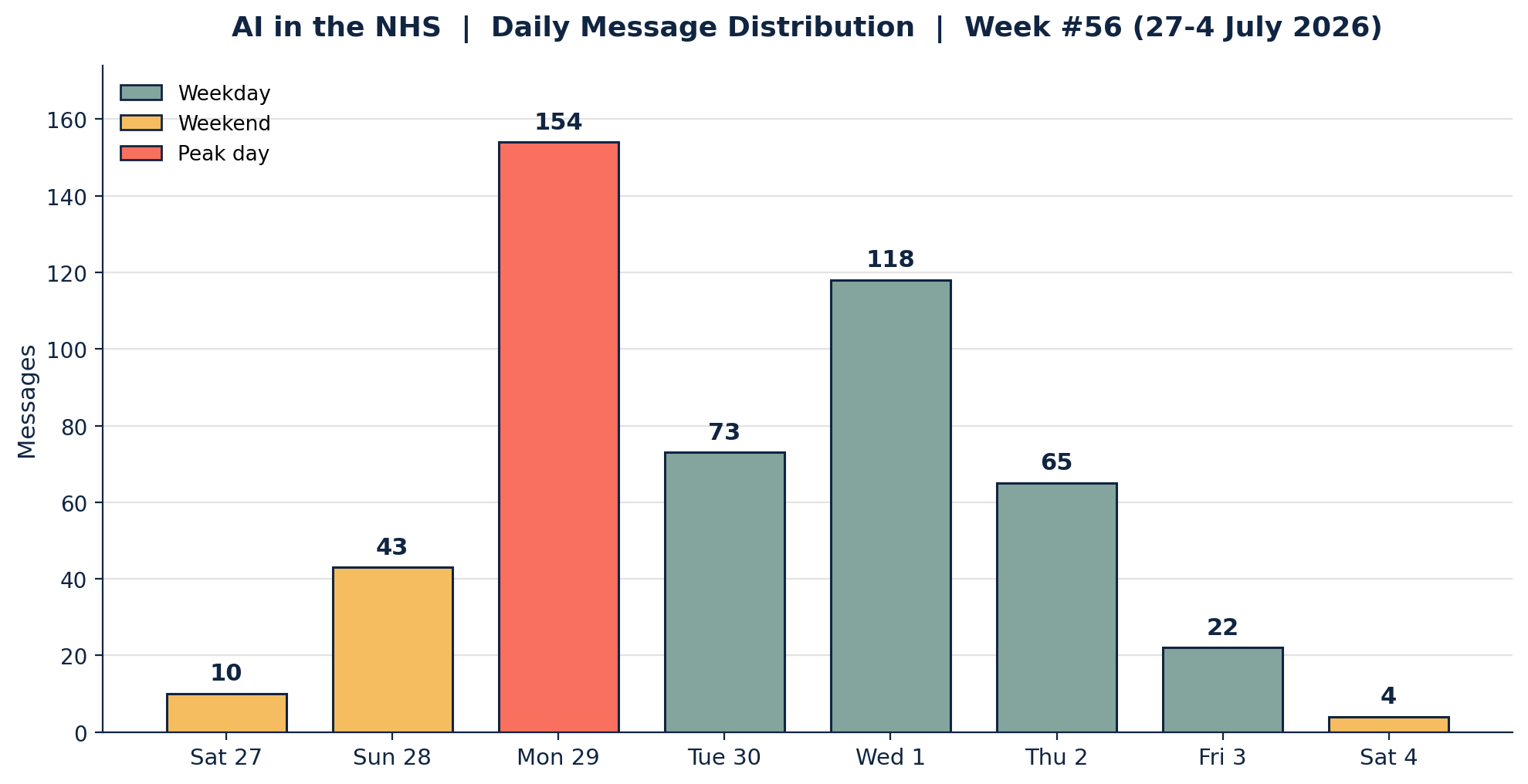
Week 56 generated 489 messages across the seven-day coverage period, with Monday 29 June the runaway peak at 154 messages, 110 of them in the afternoon alone as the AVT and deregulation threads collided. Wednesday 1 July (118) was the other heavyweight, carrying the Class IIa news and the medical-training debate, with Tuesday 30 June (73) and Thursday 2 July (65) steady behind. Weekday traffic dominated at 88.3 per cent, unusually high, with the partial Saturdays either side of the window (10 and 4 messages) leaving the working week to do almost all the talking. Sixty-five members posted at least once.
📌 Major Topic Sections
1. The AVT reckoning: evidence, hardware and who really benefits
Monday opened with a keynote claim relayed from the RCR Global AI Congress: that ambient voice technology in the ambulance service had shown a significant quality improvement in notes over human-written ones, plus a ten to fifteen per cent time saving that, scaled across the board, might eat into the outpatient backlog. The group's response was less a cheer than a cross-examination. An integrated care operations lead planted the week's flag early: "A red flag on all this for me is that no-one seems to be wondering what the impact on the clinicians is of all this extra work they'll be expected to do," and made it a matter of principle that a proper risk analysis on "the squishy meatsacks" should be a disqualifying omission. A practising clinician put the same worry personally: "I get really jumpy when people talk about using the time saved to see extra patients," because for him the time saved "goes to my cognitive headroom." A GP running an in-house AI service pressed the evidence directly: "Could NHS leadership move away from anecdotes and reference evidence please," noting that most AVT papers in the public domain still carry the vendors as co-authors, and asking for "high quality critically appraised articles... free from direct/indirect bias."
Into that scepticism arrived the week's stand-out technical contribution. A clinician and voice-technology founder, newly joined over the weekend, offered an engineer's account of why scribe quality lives or dies at the point of capture: "the source signal is the entire asset in voice technology. You can't recover detail that was never captured cleanly, however good the software downstream is." He traced loss through three stages, a cheap passive microphone, a lossy Bluetooth or phone codec ("phones run Opus... terrible for some frequencies"), and a cloud hop that compresses again, citing an IBM Watson finding that MP3 audio carried roughly ten per cent worse word-error rate than lossless. Clinical scribing, he argued, is far-field acquisition across a room, which a phone's near-field microphones "crammed centimetres apart" cannot beamform, so the long-term winner will be devices that transcribe on-chip at the source. A member with a live-sound-engineering background agreed the hardware analysis matched his own experience, and a radiology voice noted that in imaging "lossless is king", wondering whether AVT should be held to the same bar.
For all the theory, the most useful contributions were prosaic. A GP partner and committed AVT adopter offered the line the whole thread had been circling: "The number of times a cheap webcam microphone is the real reason AI scribes perform badly, only for clinicians to conclude the scribe is rubbish. Always check the microphone first." He described a practice that had paid for its own tools, kitted out consulting rooms with proper microphones and put external clinical safety governance in place, and reported the result as transformative while conceding the danger of "making us run faster on that hamster wheel." A frontline GP trialling a scribe supplied the counterweight with a catalogue of "confabulations": a summary that noted "no mention of medications" in an autism consultation, and a mishearing of "hydroxychloroquine" in a conversation about eye drops. A clinical safety and governance advocate delivered the verdict that reframed the lot: "Firstly, EVERY AVT will hallucinate. So if anyone is seeing none, I would be more worried about poor checking." The unglamorous synthesis, define an evaluation before you buy, fix the microphone, disconnect the webcam, and check the output, held all week.
2. Strip back the rules? The deregulation row and the governance answer
The regulatory temperature spiked on Monday with an HSJ exclusive reporting that regulators were "poised to strip back AI rules," and it dominated into Tuesday. Reaction divided sharply. A digital health contributor read it as calculated positioning, "deregulation is the competitive advantage that UK is seeking ahead of the EU AI Act," while others saw recklessness. The integrated care operations lead was withering: "Deregulation of patient safety interaction with AI tech is about as daft as deregulating motorcycle helmets because they get too stuffy on hot days," and refused to reconsider "before I see the detailed risk analysis of this by credible people willing to put their names and careers against it." A primary care digital policy lead widened the lens: "Surely we have to stop industrial strategy leading decisions impacting health and care?" A clinical safety advocate caught the irony that the same community pushing for basic governance keeps getting "labelled shroud wavers," even as central bodies appear to be "cutting our legs from under us."
The moderator used the moment to make his standing case. His message, he said, was simple: "You need to take control of your own governance," and while he would "extol the virtues of DCB as the most logical and applicable route in," the deeper point was that a foundation of good governance "will afford you protection, return greater control to you over your own destiny, and ultimately keep your patients and staff safe." The timing was apt, because the national review consultation on DCB0129 and DCB0160 opened the same week, and he circulated the consultation materials (including a machine-readable version "for all you good agent wranglers") and offered to build a skill that interviews members to draft their responses. A parliamentary-meeting summary shared by a digital health GP crystallised the emerging philosophy: regulation should be "a catalyst for innovation, not an obstacle," weigh the risk of not deploying a superior tool as heavily as the risk of deploying it, and above all recognise that "regulating an AI product is insufficient; the entire system, including producer, provider, professional and patient, must be regulated." The group's own long-running stand-off, between those who see Class I as too low a bar and those who now find even that too onerous, was, as one member noted drily, "a well-documented history."

3. Doing it properly meets open source's moment
If the deregulation thread supplied the anxiety, Wednesday supplied the proof of concept. News broke, via HSJ, that a UK ambient voice tool had become the first to achieve UKCA Class IIa certification, the top safety classification of its kind, and the group filled with congratulations for what everyone recognised as a hard, slow achievement. The clinician and health-tech founder behind it kept it characteristically light when asked how others might follow: "Become a masochist and it's super fun." A consultant cardiologist caught the mood, praising "the blood, sweat and tears it takes to build a company that can weather the storms of the NHS and MHRA to become an oak tree." Coming days after the "strip back the rules" story, it read as a pointed reminder that the high road exists and is walkable.
The same week made the case for a very different model. A GP running an in-house AI service seized on reporting that even Palantir was now talking up open weights and Chinese models: "Palantir the top AI and security company has endorsed Chinese models," the lesson being "open weight, keep hold of own data, be tribal." His wider argument was that open models are now "so good and close to frontier models" that the NHS and federations could "build their own AI infrastructure vs paying MSFT, Palantir, Accenture, IBM." The operations lead added the commercial realism, "quality open source equals more profit for companies using it to make money," and the cynical corollary that you need only "put a wrapper around it that says compiled in America." Anthropic, meanwhile, had a conspicuously busy week: Claude Sonnet 5 arrived narrowing the gap to Opus at lower cost, the Claude Science workbench launched (described by the moderator as "Claude Code but for science," demoed on drug discovery for PKU, with MCP connectors reaching towards online labs), and Fable returned. A member closed the circle with an older FT piece newly relevant, whose research finding, that pairing cheap open-source agents with a top-end model as an occasional "adviser" beats either alone on cost and quality, matched exactly what the group had been arguing for weeks.
4. Outsourcing reflection: AI, assessment and training
Wednesday also produced the week's most uncomfortable mirror. An academic primary care researcher shared a GP portfolio tool that expands case details into the reflective answers a trainee can paste straight into their e-portfolio, and asked the loaded question: "Is this cheating, or should deaneries and medical schools adapt to the reality of these tools coming to market?" The thread that followed was unsparing. The moderator supplied the epigram: "Here is a great example of people using AI to digitise the status quo before realising that the status quo was rubbish." A GP running an in-house AI service pushed it to the edge: "If a trainee will be outsourcing reflective thinking to AI, do we even need clinicians in the future?", while others distinguished sharply between recording reflection (a process "badly implemented at the moment") and outsourcing the thinking itself. A digital health clinician and strategist argued the tool merely exposes a deeper fragility: "so much of how the colleges operate is going to be really scrutinised and stress tested over the next few years," and suggested the incoming resident-doctor contract could "fundamentally reshape the relationship of college, member and employer." A recurring instinct was to ask whether the exercise was ever load-bearing: was reflective portfolio work "partly a self-propagating mini industry"?
The training question ran in parallel. A bioinformatician visiting a Scottish medical school open day asked what to probe about AI in the curriculum, and the answers were revealing. A veteran NHS IT specialist recalled that at his daughter's school "there wasn't much on digital health tech at all and zero on AI," except a cardiology session that told students to ignore the machine's "probable MI" readout and read the waveform themselves, an irony not lost on a group that had spent the weekend admiring exactly that raw-signal approach. Members converged on principles over tools ("responsible, trustworthy, safe... drift and bias"), reached for a driving metaphor (knowing how to drive a car is not the same as running a fleet, which is not the same as building one), and noted approvingly the appointment of a first professorial head of AI at another Scottish school. On detecting AI-written work the group was split, with cautious interest in one detector said to be more accurate than most, and firm scepticism from those who doubt any such claim will survive contact with "a resourceful student" and a risk-averse deanery.
5. From "good enough" to what works: value, population health and the FDP trust test
Thursday reset the frame with a deliberately plain question from the operations lead: asked to suggest "something AI for health and social care across a mid-large population footprint," what would you propose that you know would work, "not something new or fanciful"? The answers exposed a fault line. The moderator would "start with enhanced population-level reporting," not because the data is missing but because "the way of getting it stands in the way," and access to tools like Cowork lets people "actually use the products they've already been provided with." A primary care digital policy lead pushed back that this is the easy part: "dashboards are easy... action isn't." A clinician-innovator insisted solutions "need to start with the problems they are solving," and the group worried at the phrase "good enough" until one member observed that it too often works "to shut down pursuit of good."
Nowhere was that clearer than a bracing statins-versus-exercise exchange. A practice-based GP and digital lead argued that statins for primary prevention shift life expectancy by somewhere between minus ten and plus thirty days, against exercise worth "five to seven years," yet "in twenty years living in the UK I haven't once been encouraged to exercise by my GP practice, because QOF encourages medications and easily measured medicalised outcomes." A digital health technologist supplied the population-health counter, that statins are so cheap "it is more cost effective to offer it to pretty much everyone than burn the tokens to ask AI to find the patients who may benefit most," the very "fag-packet maths" used to justify blanket intervention. The same appetite for value-for-effort drove a run on prescribing-support software, with several practices describing switching it off over the seconds-per-script cost and one member noting it could be disabled through organisational settings, with a pointed reminder to check the deploying organisation's own DCB0129 documentation. The week closed on trust in the biggest data programme of all: reporting that a metro mayor was set to ditch Palantir, a London hospital waiting-list story, and, on Friday, a watchdog investigation into NHS England's claims about the Federated Data Platform's effectiveness. Set beside a warning that a cyberattack is now a bigger risk to the NHS than another pandemic ("Covid never closed an entire hospital, a really bad cyberattack could"), it made for a sober finish to a week that had started with microphones.
😄 Lighter Moments
For all the governance and geopolitics, the group's humour held. The moderator introduced a bioinformatician who joined mid-week with a firm "NO SPECIAL TREATMENT," only for the group to adopt them instantly as the trusted source of "the goss and secret stuff." A cheerful cross-border skirmish followed, with one member offering "missionary duties in helping the poor English folk with their NHS" and another crediting the Scots with "fixing Hadrian's Wall and making a good job of it." Reports from corporate hospitality raised eyebrows and life goals in equal measure: an IBM office boasting "an AI wine fridge to help you choose what you want to drink," and a City law firm where "lifelong grudges get held over missing teaspoons." A shared post on the limits of AI receptionists produced the week's finest mishearing, "I was kept up all night with heart palpitations" faithfully transcribed as "I was kept up all night with a hot politician." One member confessed to reading a pirate-flavoured message "in a pirate voice, adding a couple of AARRRs at the start and end," and, on the discovery that a new AI scribe struggled in hot weather, another diagnosed the culprit as a noisy cooling fan. Amid a run of Anthropic launches, the standing gag about being throttled by usage limits resurfaced ("gonna absolutely MAX the usage until then, everything is getting a security audit"), alongside the eternal question of whether a message arriving at 3am was "the real you playing with Fable, or Fable impersonating" you.
💬 Quote Wall
"Always check the microphone first. It fixes the vast majority of problems in my experience." — A GP partner and committed AVT adopter
"Firstly, EVERY AVT will hallucinate. So if anyone is seeing none, I would be more worried about poor checking." — A clinical safety and governance advocate
"Deregulation of patient safety interaction with AI tech is about as daft as deregulating motorcycle helmets because they get too stuffy on hot days." — An integrated care operations lead
"You need to take control of your own governance... it will return greater control to you over your own destiny, and ultimately keep your patients and staff safe." — The group moderator, on the deregulation story
"Here is a great example of people using AI to digitise the status quo before realising that the status quo was rubbish." — The group moderator, on the GP portfolio tool
"The source signal is the entire asset in voice technology. You can't recover detail that was never captured cleanly, however good the software downstream is." — A clinician and voice-technology founder
"I get really jumpy when people talk about using the time saved to see extra patients. The time saved goes to my cognitive headroom." — A practising clinician, on AVT
"Dashboards are easy... action isn't." — A primary care digital policy lead, on population health
📎 Journal Watch
Academic Papers and Key Studies
📎 Closing the AI liability gap – Medical Protection Society. A policy paper (with a companion blog) shared into the recurring worry that a widening gulf between AI and the law could leave the NHS and doctors exposed to claims. Read more
📎 Deep neural networks applied to raw ECG waveforms – Nature. Circulated with the tagline "it's not all about LLMs," a worked example of what can be done with raw signal versus interpreted output, and a touchstone for the week's AVT fidelity debate. Read more
📎 Tirzepatide and cardiovascular outcomes – The BMJ. Shared in the statins-versus-lifestyle thread as a prompt to apply the same cost-effectiveness logic to the newer weight-loss agents. Read more
📎 Will US control of AI affect health outcomes as drug pricing has? – The BMJ. A "punchy" Saturday closer drawing a parallel between pharmaceutical pricing power and concentrated control of AI. Read more
📎 Advertising-sponsored products in LLM outputs – arXiv. A preprint on the conflict between user and company priorities when models suggest expensive, ad-sponsored products, more so where high socioeconomic status is inferred. Read more
📎 Pairing open-source agents with frontier "advisers" – Fireworks AI. The research behind Thursday's FT-anchored argument that cheap open agents plus a top-end model as occasional adviser can beat either alone on cost and quality. Read more
Industry and News Articles
📎 Regulators poised to strip back AI rules – HSJ. The week's pivotal, and most contested, story, read variously as bold competitive positioning and as deregulating patient safety. Read more
📎 UK AI tool first to get top safety certification – HSJ. The report that a UK ambient voice tool had become the first to achieve UKCA Class IIa, held up all week as proof that "doing it properly" is achievable. Read more
📎 Watchdog launches investigation into NHSE's FDP effectiveness claims – HSJ. Friday's development in the Federated Data Platform trust saga, alongside reporting that a metro mayor was set to drop Palantir. Read more
📎 Contractor assessed its own service in ICB procurement – HSJ. Filed by the group under "all you need to understand why NHS procurement often gets it badly wrong in one article." Read more
📎 Cyberattack risk to the NHS "dramatically accelerating" – HSJ. The source for Friday's sober coda that a serious cyberattack now outranks another pandemic as a threat to NHS continuity. Read more
📎 Anthropic is "eating Palantir's lunch" – Yahoo Finance. Market-side colour for the week's running Palantir-versus-open-models thread. Read more
📎 How much value is AI really creating? – Financial Times. John Burn-Murdoch's piece, resurfaced for its electricity-era analogy and its open-source-plus-adviser research finding. Read more
📎 UpDocs AI gets FDA nod as a "concierge doctor between visits" – Wall Street Journal. Shared at the top of the week as a marker of how fast the between-visits AI space is moving. Read more
📎 Anthropic moves into AI-driven drug development – STAT. Context for the Claude Science launch and its life-sciences ambitions. Read more
Technical Resources and Guidelines
📎 Claude Science (AI workbench) – Anthropic. The week's headline product launch, described as "Claude Code but for science," with connectors for life-science platforms and a PKU drug-discovery demo. Read more
📎 Claude Sonnet 5 – Anthropic. The mid-tier model that "narrows the gap" to Opus at lower cost, with a much-discussed tokeniser cost profile across languages. Read more
📎 Why audio compression format impacts speech-to-text accuracy – IBM Watson (Medium). The reference behind the founder's signal-fidelity case, quantifying the word-error penalty of lossy codecs. Read more
📎 The AI Readiness Checklist – CERSI-AI. Surfaced in the hunt for an up-to-date successor to the ageing NHSX "Buyer's Guide to AI," which several members want NHSE to own and refresh by use case. Read more
📎 NHS AI Knowledge Repository – NHS England. Offered as the current best home for AI buyer guidance, alongside a wish for "a single document, old style." Read more
📎 Qwen Robotics Suite – Qwen. An open robotics stack shared into the new member's physical-AI and on-device processing thread. Read more
Policy Documents and Official Reports
📎 National review of clinical risk management standards (DCB0129 and DCB0160) – NHS England engagement. The consultation that opened this week on the very standards the group keeps advocating; the moderator shared the materials and offered a skill to help members respond. Read more
📎 AI Airlock Phase 2 programme report – MHRA. Cited for its recommendation 5, that products falling outside device status still sit within a shared ecosystem interest in safety and accountability. Read more
📎 Generative AI and the MRCGP WPBA – RCGP. The college's own position, shared as the reference point for the trainee-portfolio and reflection debate. Read more
📎 Help shape how health data is used across the NHS – DHSC / kscopehealth. A live engagement programme on patient data policy and the single patient record, circulated for GPs and practice staff to contribute. Read more
🔭 Looking Ahead
The DCB0129/0160 consultation is the concrete action item: with the national review open, expect the group to keep sharing responses, and to take up the offer of a drafting skill to make submitting easier. The "strip back the rules" story will run until the detail emerges, and members will be watching whether the AVT working groups within the wider commission land on Class I, Class II or "wait and see." The freshly certified Class IIa scribe sets a marker others will be measured against, while the open-weights argument (sharpened by Palantir's apparent turn and Anthropic's Sonnet 5, Claude Science and Fable releases) points towards federations and practices building more of their own stack. A federation network has asked for AI speakers for a members' learning session in late July, an anonymous academic survey on AVT governance in UK primary care is open to contributors, and the Palantir and Federated Data Platform trust question now has a watchdog investigation attached to it. Underneath it all, the training debate is only beginning: portfolios, reflection, detection and the incoming resident-doctor contract are set to test how colleges and deaneries operate for years to come.
🧬 Group Personality Snapshot
This is a community that will interrogate a keynote's headline number before it will applaud it, then spend an afternoon on microphone geometry and codec loss because the details are where safety actually lives. It prizes independent, conflict-free evidence, distrusts anything sold as "good enough," and reaches instinctively for governance you own rather than rules handed down, yet it celebrates a hard-won Class IIa certification as warmly as it punctures a self-assessing procurement. It is comfortable holding two truths at once: that AVT can be genuinely transformative in a well-run practice, and that most of the narrative around it is about squeezing clinicians harder. It swaps raw-signal ECG papers and statins-versus-exercise arithmetic with the same energy it brings to a mishearing about a "hot politician," a City firm's teaspoon grudges, and an IBM wine fridge. Above all it keeps returning to the same test it applied to the week's shiny launches and its scariest headlines alike: not what the technology can do, but what it does for patients, for frontline workload, and for the people expected to stand behind it when something goes wrong.
APPENDIX A: Detailed Activity Analytics 📊
📬 Total Messages: 489
📈 Peak Day: Monday 29 June (154 messages)
🔥 Most Active Period: Monday afternoon (110 messages)
💬 Average / Active Day: 61 messages
🏖️ Weekend Activity: 11.7% (57/489)
💼 Weekday Activity: 88.3% (432/489)
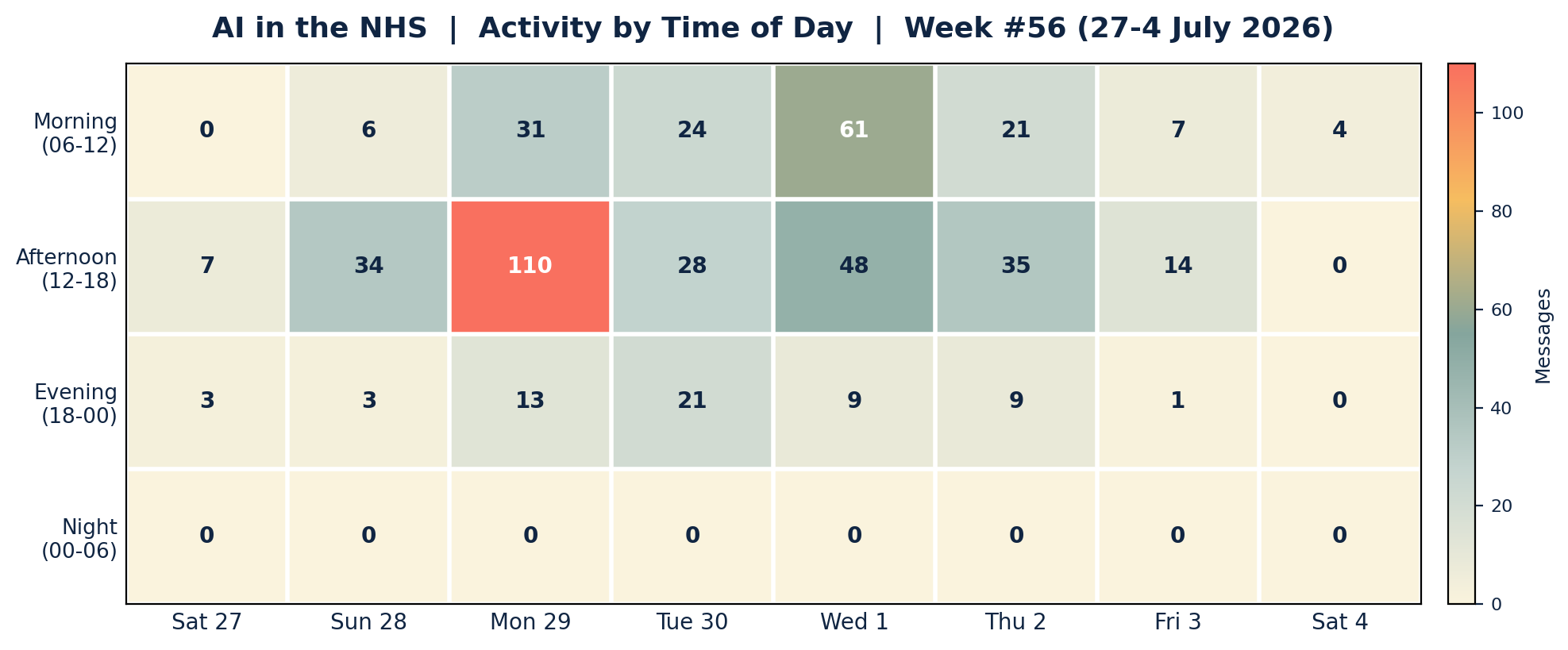
Engagement was overwhelmingly a weekday-daytime affair. Monday carried the week, its morning (31) and afternoon (110) both heavy as the AVT quality debate, the hardware deep-dive and the "strip back the rules" story overlapped. Wednesday morning (61) was the single busiest morning, driven by the Class IIa news and the medical-training thread. Evenings were muted by this group's standards and night-time activity was nil across all eight days, an unusually clean sleep record for a community that often talks past midnight.
APPENDIX B: Enhanced Statistics
Unique Contributors: 65 group members posted at least one message this week, out of the group's wider membership of around 800. The 15 most active below account for 367 of the 489 messages (75.1 per cent), with a long tail of occasional and one-off contributors making up the remaining 122 messages.
Top 15 Contributors (Role Descriptors Only):
1. Digital Health & Clinical AI Specialist (Group Moderator): 83 messages
2. GP running an in-house AI service: 34 messages
3. Integrated care operations lead: 32 messages
4. NHS IT and informatics specialist: 29 messages
5. Clinical safety and governance advocate: 28 messages
6. GP partner and committed AVT adopter: 24 messages
7. Clinician and voice-technology founder: 23 messages
8. Health-tech industry contributor: 19 messages
9. Digital health technologist: 17 messages
10. Academic primary care researcher: 16 messages
11. Digital health GP and data scientist: 16 messages
12. Digital health contributor: 12 messages
13. Digital health clinician and strategist: 12 messages
14. Frontline GP trialling an AVT scribe: 12 messages
15. Health-tech contributor: 10 messages
Hottest Debate Topics:
1. 🔥🔥🔥 AVT quality, evidence and signal fidelity (Mon, with Sun and Tue tails)
2. 🔥🔥🔥 "Regulators poised to strip back AI rules" and the governance answer (Mon-Tue)
3. 🔥🔥 Class IIa certification, open weights and Anthropic's launches (Wed)
4. 🔥🔥 AI, trainee reflection, portfolios and medical-school curricula (Wed)
5. 🔥🔥 Population health, "good enough" and statins versus exercise (Thu)
6. 🔥 Palantir, the FDP and the procurement trust question (Thu-Fri)
7. 🔥 Cyber risk versus pandemic risk to the NHS (Fri)
Discussion Quality Metrics:
• External resource sharing: more than 35 unique links across the period, spanning peer-reviewed papers, official consultations, trade press, vendor launches and open-source tooling
• Evidence base: strong, anchored by a Nature raw-waveform paper, two BMJ papers, an MPS liability policy paper, the MHRA AI Airlock Phase 2 report and the DCB0129/0160 consultation
• Constructive challenge: high, with the AVT-evidence, deregulation and statins threads all featuring sustained, respectful disagreement grounded in data and frontline experience
• Breadth of participation: 65 unique contributors, though weighted towards a weekday-daytime core, with a genuinely long tail of one-off voices
Cross-Expertise Engagement:
The week drew GPs and GP partners, practice managers, radiology and hospital voices, NHS IT and information-security specialists, informaticians and bioinformaticians, operations and federation leads, health-tech founders and hardware engineers, medical educators and academic researchers, and clinical-safety and policy leads. The most cross-disciplinary thread was Monday's AVT debate, which pulled clinical, engineering, regulatory, operational and commercial perspectives into a single conversation. Several new members were welcomed during the week, including a clinician and voice-technology founder and a bioinformatician.
APPENDIX C: Daily Theme Summary
Saturday, 27 June 2026 (from 09:00)
Primary Theme: Quiet handover and the GLP-1 aside Key Discussion: Newsletter #55 went out to the group, and a light Saturday turned on the newer, centrally-acting GLP-1 compounds and their effects on peripheral inflammation, with a reminder that "it's not all about LLMs." Secondary Discussions: A US FDA nod for a "concierge doctor between visits" tool; a Nature ECG paper on raw waveforms. Notable: A gentle start (10 messages) before the working week took over.
Sunday, 28 June 2026
Primary Theme: Liability, translation and a new voice-hardware voice Key Discussion: An MPS paper on closing the AI liability gap set the tone, while a newly-joined clinician and voice-technology founder began what would become the week's defining hardware thread, and members swapped RAG and embedding learning resources. Secondary Discussions: A medical-translation paper; deep neural networks on raw ECGs; an open robotics suite; agentic primary care with PPG involvement. Notable: The moderator introduced a bioinformatician to the group, "NO SPECIAL TREATMENT."
Monday, 29 June 2026
Primary Theme: The AVT reckoning and the deregulation bombshell Key Discussion: A congress claim of AVT quality gains and time savings met hard questions about clinician impact, conflict-free evidence and signal fidelity, colliding in the afternoon with an HSJ exclusive that regulators were poised to strip back AI rules. Secondary Discussions: Microphone quality and confabulations; open-sourcing AVT; on-chip transcription; personal-device data risks; AI receptionist limits. Notable: The week's peak by a distance (154 messages, 110 in the afternoon).
Tuesday, 30 June 2026
Primary Theme: Governance as the answer, and a busy Anthropic Key Discussion: The moderator urged members to take control of their own governance with DCB as the route in, as the deregulation debate matured into a "new philosophy for regulation," and Claude Sonnet 5 and the Claude Science workbench launched. Secondary Discussions: The ageing NHSX Buyer's Guide and CERSI-AI checklist; the DCB0129/0160 consultation opening; a Kings Fund AVT panel. Notable: "Deregulation... about as daft as deregulating motorcycle helmets."
Wednesday, 1 July 2026
Primary Theme: Class IIa, open weights and outsourced reflection Key Discussion: A UK ambient voice tool became the first to reach UKCA Class IIa, celebrated as "doing it properly," while a GP portfolio tool ignited a debate about outsourcing trainee reflection to AI and what medical schools should teach. Secondary Discussions: Palantir endorsing open and Chinese models; NHS procurement self-assessment; Claude Science and Fable; the Sonnet 5 tokeniser cost profile. Notable: The second-busiest day (118 messages).
Thursday, 2 July 2026
Primary Theme: What actually works, and the value question Key Discussion: A deliberately plain "what would you deploy that you know works" prompt exposed the gap between easy dashboards and hard action, running into a statins-versus-exercise argument about where health value really lies. Secondary Discussions: Sovereign AI and data centres; "good enough" as an enemy of good; prescribing-support software and collective action; the FT electricity analogy. Notable: A metro mayor reported to be set to drop Palantir.
Friday, 3 July 2026
Primary Theme: Trust, the FDP and cyber risk Key Discussion: A watchdog investigation into NHS England's Federated Data Platform effectiveness claims, alongside Foxglove reporting, met a warning that a serious cyberattack now outranks another pandemic as a threat to NHS continuity. Secondary Discussions: GP data-engagement programme; a contested investor claim about a leading AI firm; short-dated pharmacy stock as a false COVID signal. Notable: "Covid never closed an entire hospital, a really bad cyberattack could."
Saturday, 4 July 2026 (to 09:00)
Primary Theme: A punchy close Key Discussion: A BMJ piece asked whether US control of AI could shape health outcomes as drug-pricing power has, and a preprint on advertising-sponsored LLM outputs highlighted the conflict between user and company interests. Secondary Discussions: An Independence Day aside. Notable: Coverage closes at 09:00 on Saturday 4 July.
AI in the NHS Weekly Newsletter is produced by Curistica Ltd for members of the AI in the NHS WhatsApp community. All contributors are anonymised. Views expressed are those of individual community members and do not represent any organisation.