Executive Summary
If last week was the group's first birthday, this week was the morning after, and the conversation turned sharply to the gap between the promises being made about AI in the NHS and the machinery underneath them. Monday opened with the announcement that 500,000 NHS staff would receive Microsoft Copilot, alongside eye-watering savings claims, and the group spent the day picking apart what "certified as safe" actually means and whether a tool that cannot touch the clinical record can really free up clinician time. By Tuesday the mood had darkened into liability: a GPonline piece on the AI "liability gap" collided with a member's real-world question about a therapeutic chatbot hiding behind a "beta, for testing only" disclaimer, and the answer from the group was unanimous and unforgiving. Midweek brought the long-trailed National Commission and MHRA reports on regulating AI in healthcare, which one member condensed into ten findings that read like a summary of this group's own preoccupations: proportionate risk, post-market surveillance, shared liability, human-in-the-loop, and AI literacy.
Running underneath all of it was a new Anthropic model, "Mythos" (consumer name "Fable"), which arrived to genuine awe and ended the week with the United States ordering its access blocked for any foreign national, including Anthropic's own overseas staff. The group read that as regulatory capture and a fresh argument for sovereign and open-source models. Between the heavy themes there was room for Scotland's World Cup hopes, an underwater datacentre, a creepypasta hospital game built overnight, and a long, fond argument about why the NHS keeps paying the big four consultancies for slides it could have written itself. Four hundred and fifty-four messages across seven days; here are the threads that shaped them.
Activity at a Glance
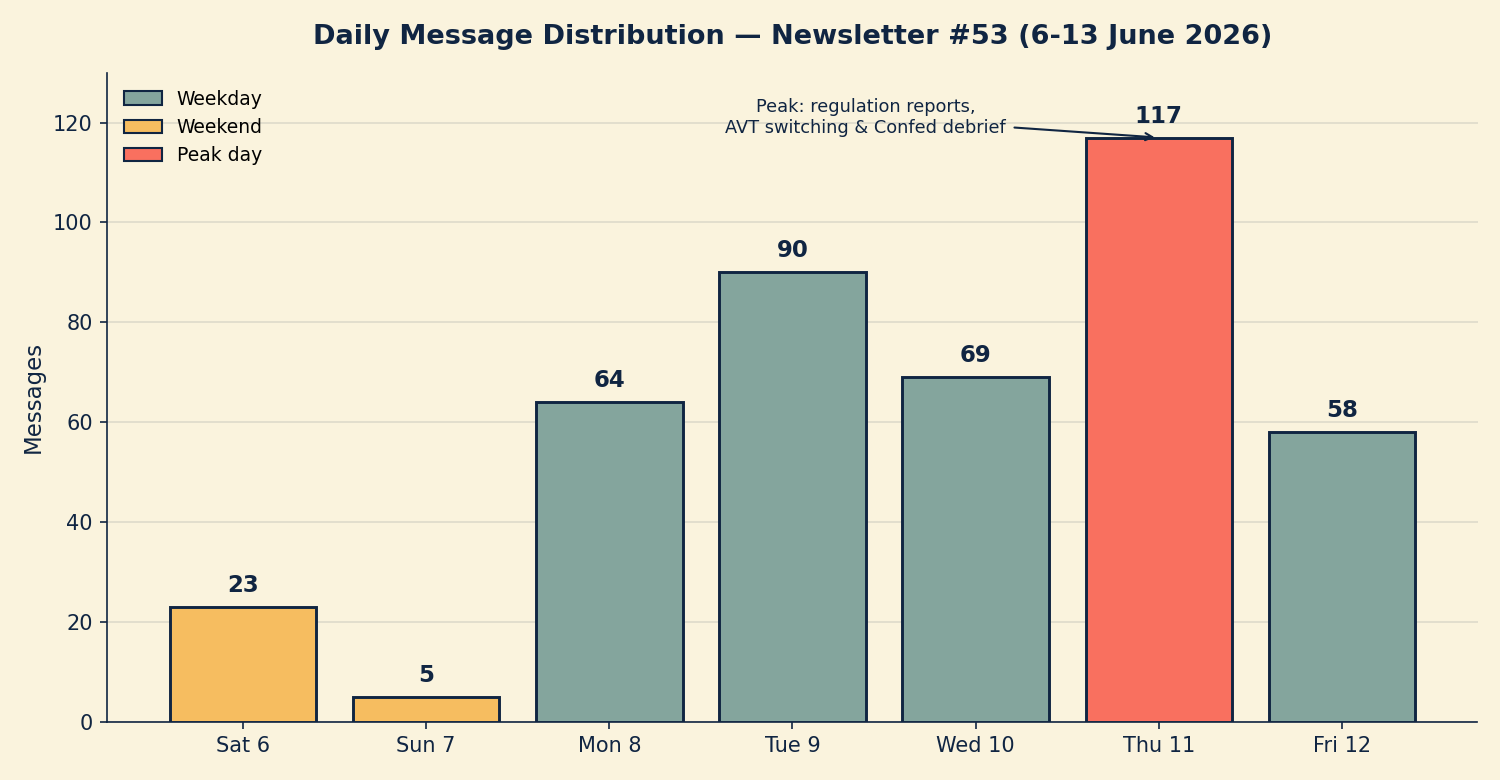
Week 53 generated 454 messages across the seven-day coverage period. Thursday 11 June was by far the busiest day (117 messages), driven by an evening that ran the regulation reports, AVT switching, GP2GP data and NHS Confed Expo debriefs all at once. Tuesday 9 June was the second peak (90 messages) around the liability debate and the Mythos launch. The weekend bookends were quiet after last week's first-birthday special, with Sunday 7 June the quietest day at just 5 messages. Weekday traffic dominated at 87.7 per cent, a noticeably office-hours week.
📌 Major Topics
1. Copilot for 500,000: the savings claim meets the safety question
The week began with the announcement that half a million NHS staff would receive Microsoft 365 Copilot, trailed against a 2025 trial promising "unprecedented" time and cost savings. The group was sceptical from the first message. An agentic-primary-care GP claimed, citing reports, that even Microsoft's internal teams prefer Claude, and questioned how the NHS could be "somehow convinced that Copilot will deliver £213 billion of annual savings." A trust informatician offered the counterweight: in his non-clinical world Copilot had "completely removed the usual note-taking activities for project managers and management," largely because of its tight integration with Teams.
That split, between administrative gains and clinical reality, ran through the whole thread. A frontline GP put it plainly: "I'm struggling to think what it could do for me in its current state that would save me 43 minutes a day." An integrated care operations lead agreed, suspecting "the sacrifice would be quality over quantity." The recurring obstacle was integration, with one member pointing out the tools "cannot integrate with SystmOne," and another noting that even Power Automate is not in the standard NHS tenant.
The group's clinical-safety instincts surfaced quickly. When a trust informatician said the data "sits inside the NHS tenant, so certified as safe," the group moderator drew the crucial distinction: a Copilot context pull "can come from repositories of data that may hold information that isn't intended for wider use." The informatician clarified he had said "certified as" safe, not safe. An operations lead wondered aloud about "the informed consent status of whoever signed that one off." For a more sober read than the press release, members pointed to the DBT Copilot pilot evaluation report.
2. The liability gap, and the "beta, for testing only" defence
Tuesday's centrepiece was a GPonline article warning that GPs are exposed to clinical negligence claims through an AI "liability gap." An operations lead, who has flagged this for months, summarised the danger: suppliers limit liability everywhere, while courts give registered professionals "zero latitude" for missing AI errors such as hallucinations. The particular peril, he stressed, is that "the vast majority of GP practices are unlimited liability partnerships." A medicolegal adviser clarified that NHS Resolution's Clinical Negligence Scheme for General Practice would cover liabilities in tort for personal injury, but the group noted this covers patient harm only, leaving GMC referrals and other implications open.
That theory became concrete when a hospital innovation lead put a general question to the "hive mind": can a developer release a therapeutic AI to the public behind a website disclaimer reading "beta platform for testing only"? The reply from a clinical AI governance specialist was immediate: "Absolutely not." A clinical governance advisor set out the principle, that any such tool needs "an intended use statement, determine their device class, and they need a DCB0129 for starters," and that where a tool meets the definition of software as a medical device a disclaimer cannot exempt it from regulation. The group's consensus was that a direct-to-patient health app faces stricter liability still, potentially engaging the Unfair Contract Terms Act, and that "beta" or "not for real use" labels offer little cover. A digital health founder set out the MHRA's enforcement powers, including compliance, suspension and safety notices, and the fact that breaching the regulations can carry "imprisonment up to 6 months, or a fine, or both."
3. The National Commission and MHRA reports: the group, written up
Midweek delivered the documents the group has been waiting for: the National Commission into the Regulation of AI in Healthcare's call-for-evidence findings, and the MHRA's "landmark report" on public views. The group moderator ran them through the new model and posted a condensed set of ten findings, which he noted "mirrors the opinions expressed in this group": a proportionate, risk-based, lifecycle approach; continuous post-market surveillance because "one-off approvals are inadequate"; liability shared across manufacturer, provider and clinician; human oversight retained, with AI as decision support not replacement; transparency and plain-English explainability; strong public concern about commercial use of NHS data; robust AI literacy "including for CSOs and governance teams"; and a call for a centralised national AI incident reporting system.
The quantitative split was striking. On data governance, 82 per cent of patients said the framework was insufficient against 48 per cent of industry calling it sufficient; on liability, 75 per cent of patients said existing laws are unfit for AI versus 15 per cent of industry. "Industry was consistently the most satisfied group; patients and public consistently the least." The moderator's reading was that "the direction of travel feels very much towards better governance, oversight and training versus regulatory change," underlining how important getting your own governance framework in place will be. A radiology AI lead immediately spotted the tension for his field: what does "decision support, not decision replacement" mean for autonomous high-confidence normal reporting in radiology?
4. Device classification: Class I, Class II, and which way the MHRA is leaning
The reports reignited a long-running classification debate. A digital health founder reported that the draft NHS AI framework spec demands "Class 2 as a minimum," which the moderator noted "runs in contradiction to MHRA," given the regulator's apparent trend towards treating standalone software as Class I. A radiology AI lead pushed back, reporting that he had heard the MHRA "privately briefing that AVTs better shape up for Class II," and that "there may be different tribes inside the MHRA." A regulatory specialist predicted the market would settle it regardless: once one major provider achieves Class IIb with a notified body, it will "push the narrative that all AVTs should be at a minimum the same class as theirs," a point underlined by news that one scribe vendor is now MDR Class IIa certified.
The pragmatic consensus leaned towards EU alignment. The regulatory specialist argued the "highest yield move" for anyone with EU presence is to seek a CE mark, since EU MDR is tighter than UKCA on SaMD and near-complete alignment would let the UK regulator "almost outsource the enforcement to the EU." A separate strand untangled the NHS Shared Business Services framework, which turned out, after its 399th clarification response to bidders, not to be NHS-specific at all but the generic Government AI assurance classification. "Mystery solved."
5. Mythos and Fable: awe, neologisms, and a US export block
The week's other main character was a new Anthropic model, internally "Mythos" and consumer-facing "Fable." The reception was close to reverent. "Good grief this is good," wrote the moderator within minutes of release; a GP developer called it "an exceptional model" mid code-review and admitted he would "be sad when this comes off plan." A tech-literate GP relayed that Simon Willison had described it as "something of a beast" and, two days later, "relentlessly proactive in pursuit of its goals." The moderator confirmed it had done "exceptionally smart things," all while "speaking in an increasingly opaque manner," noticing it using neologisms such as "questals" and "vendoring" a Python library, "baroque language that kind of makes sense."
The economics drew the sharpest wit. With reports that the model burns roughly twice the tokens of its predecessor, an agentic-primary-care GP joked that "I thought Claude was on the way to becoming GOD," prompting the moderator's instant classic: "The more tokens you sacrifice, the more likely they are to grant your prayer." Then on Saturday the tone changed: the US government issued an order to suspend all access to Fable and Mythos "by any foreign national, whether inside or outside the United States, including foreign national Anthropic employees," and Anthropic complied. "Regulatory capture has begun," wrote one member. Others read it as a gift to open-source and sovereign models, the moderator observing that "once again, the US stimulates countries around the world to accelerate their independence from dependence on, checks notes, the US."
6. Sovereignty, local models and the data duopoly
The export block landed on ground the group had already been digging all week. An edge-AI engineer opened Saturday with NVIDIA's new streaming ASR model that "could run on edge with only 1 to 2GB and CPU, no GPU needed," arguing small on-prem models are the direction of travel and could "really disrupt cloud provision of AVT" while keeping inference out of the USA. By midweek the moderator had his 64GB MacBook running local models via LM Studio, taking recommendations for Qwen 3.6 and Gemma 4, and describing how a Subject Access Request had let him pull his own full medical record into structured form to "finally let rip" with an offline model.
That prompted a rich exchange on GP data portability. An interoperability veteran defended GP2GP as "a very good example of standardisation" born before the duopoly, while another interoperability specialist countered that "huge amounts of data are lost with every GP2GP transfer" and that the suppliers already have the mechanisms, through GP Connect structured records and forthcoming standards, to do far better. He ran a poll on how many records became "Transfer Degraded" in a year, with the group split between 35 million and 350 million. A consultant lamented what he saw as the suppliers' long resistance to genuine interoperability, and the failure of central bodies to hold them to account.
😄 Lighter Moments
For all the regulation and liability, the group kept its sense of fun. Scotland's World Cup qualification produced a run of self-deprecating Caledonian humour, from "Obviously Scotland will win" to "I'll take things that will never happen for 1000" and the inevitable consolation of the "Best Fans award as usual." A member set up a prediction league named "Hooferoo" and invited the group to "infiltrate it with AI puns."
The moderator's late-night experiment with the new model produced "Liminal Hospital," a creepypasta walking simulator set in "St Curwens," shared with the warning that "if your lights dim or the stars start going out, it wasn't me." The group's verdict: "Never seen a hospital this clean," and "brings back those Second Life vibes." A GP innovator livened up the NHS Confed Expo by flying a drone over the exhibition floor, earning the line of the week: "You are the only person I know who would take a drone to an exhibition." And in the running gag about how Anthropic might ever turn a profit, one member summarised the route to unlimited tokens as needing only "Claude Code, an API key and Coutts account details."
💬 Quote Wall
"We are the teeth." — Group moderator, on who actually enforces clinical safety
"The more tokens you sacrifice, the more likely they are to grant your prayer." — Group moderator, on AI economics
"Moat is largely retraining and redoing all the safety case." — GP developer, on the real cost of switching AVT providers
"Probabilistic models gonna probabilistic." — Group moderator, on why new tools must always be re-checked
"'Could' has done a lot of vapourware-like heavy lifting in the healthtech space for a long, long time. Would love to witness the shift from could to does." — Health tech consultant
"Leaders can take all the risks they want. After all, we will be the ones thrown under the proverbial buses." — Health tech consultant, on the call for more risk-taking
"This competition is accelerating us very fast through the mess-around phase and to the find-out phase." — Global digital health specialist
"The NHS would be a whole world better if people driving change were judged against the output rather than just how good they are at making presentations about it." — Integrated care operations lead
📎 Journal Watch
Academic Papers and Key Studies
📎 OpenEvidence versus frontier models for health purposes – Nature Medicine. The study reported that frontier LLMs (GPT-5.2, Gemini 3.1 Pro, Claude Opus 4.6) outperformed dedicated clinical AI tools such as OpenEvidence and UpToDate Expert AI in its evaluations, a finding the group found striking given the constellation-versus-foundation-model debate Read more
📎 Evaluation of clinically-focused AI chatbots for drug information questions – JACCP. A study assessing how well clinical AI chatbots answer medicines queries, prompting a pharmacist-side discussion on whether the BNF or RPS should build semantic search over their own curated corpus Read more
📎 AI, the "learned intermediary" and history-taking – npj Digital Medicine. A paper raising whether clinicians should now ask patients "have you used an AI chatbot for advice about your medications or symptoms?" and revisiting the spectre of malpractice for not consulting AI Read more
📎 BMJ research article (9 June 2026) – The BMJ. Shared into the Tuesday discussion on evidence and AI in practice Read more
Policy Documents and Official Reports
📎 National Commission into the Regulation of AI in Healthcare: call-for-evidence findings – gov.uk. The headline policy document of the week, condensed by members into ten findings spanning proportionate regulation, post-market surveillance, shared liability and AI literacy Read more
📎 MHRA landmark report reveals public views on AI in healthcare – gov.uk. The companion MHRA report, notable for the sharp divergence between patient and industry views on data governance, liability and how loose or tight the framework is Read more
📎 Beyond Productivity: AI and NHS workforce implications – UCLPartners. Commissioned by NHS England London Region, the report argues AI does not simply reduce work but redistributes it, creating new duties around checking, validation and oversight, and calls for a workforce-centred approach Read more | Read more
📎 500,000 NHS staff to get new AI tools – NHS England. The Copilot rollout announcement that opened the week, paired with the 2025 trial press release Read more
📎 Microsoft 365 Copilot pilot: DBT evaluation report – gov.uk. Offered as a "much more thoughtful and comprehensive view" than the savings headlines Read more
📎 Medical device stand-alone software including apps (MHRA guidance) – gov.uk. Cited to set out MHRA enforcement powers, from compliance and suspension notices to potential imprisonment for breaching the regulations Read more
📎 Introduction to AI assurance – gov.uk. The generic Government AI assurance classification that the NHS Shared Business Services framework turned out to reference Read more
Industry and News Articles
📎 GPs exposed to clinical negligence claims due to AI "liability gap" – GPonline. The article that anchored the liability debate, warning of the gap between supplier liability limits and the latitude courts give professionals Read more
📎 Take more risks with new technology, urges health secretary – HSJ. The new health secretary's call for more risk-taking, which divided the group between "we are the teeth" and "we will be thrown under the buses." Read more
📎 Digital chief: NHS AI ban is "criminal"– HSJ. The counterpoint headline, paired with the above to show the policy mood Read more
📎 The first casualty of the great AI redundancy: the big four – Financial Times. The article that launched a long thread on consultancy "AI slop," repackaged reports and why the NHS keeps paying for them Read more
📎 Anthropic restricts Fable and Mythos access – Anthropic. The Saturday announcement that the US had ordered access blocked for foreign nationals, including Anthropic's own overseas employees Read more
📎 Anthropic "made the wrong tradeoff" on guardrails – Business Insider. Anthropic conceding it may have overdone the safeguards, explaining why the model kept reverting to an earlier version for some users Read more
📎 You can now get a religious exemption from using AI at work – Futurism. Shared half in jest as a possible route for clinicians if Crown indemnity does not cover AI use Read more
📎 World's first wind-powered underwater datacentre starts operating in China – The Guardian. The trigger for a tangent on data-centre heat dissipation, sea batteries and "Day After Tomorrow" jokes Read more
Technical Resources and Commentary
📎 What it feels like to work with Mythos – One Useful Thing. Ethan Mollick's impressed first take on the new model, including the games he built with it Read more
📎 Claude Fable 5: "something of a beast" and "relentlessly proactive" – Simon Willison. Two posts that the group used to calibrate expectations of the new model's behaviour Read more | Read more
📎 NVIDIA Nemotron streaming ASR (0.6b) – Hugging Face. The edge-deployable speech model floated as a potential open, on-prem basis for NHS ambient voice Read more
📎 Gemini Diffusion – Google DeepMind, and Gemma 4 12B – Google. A new diffusion model that generates output in self-correcting blocks, plus a home-GPU-friendly open model, both discussed in the local-models thread Read more | Read more
📎 Agents' Last Exam leaderboard – agents-last-exam.org. Cited to temper automation hype: the best agentic pass rate sits at 26 per cent Read more
🔭 Looking Ahead
NHS Confed Expo wrapped midweek and HLTH Europe runs in Amsterdam next week, with several members attending and a discount code shared in the group. A CSO "Coffee and Chat" community continues to meet monthly for clinical safety officers and engineers. The export block on Fable and Mythos will keep the sovereignty and open-source conversation running hot, and members are watching to see whether the MHRA settles its apparent internal split on device classification before the National Commission reports in full. Several consultations remain open, including an NHS health-data engagement exercise and an ABHI apps-and-wearables strategy seeking input from commissioners and implementers.
🧬 Group Personality Snapshot
This is a community that treats a regulator's report as required reading and then argues about it line by line, but never loses the plot of why it matters: real patients, real liability, real practices on unlimited liability partnerships. The week showed the group at its most characteristic, swinging from MHRA enforcement powers to a creepypasta hospital game and back without missing a beat, equally happy to dissect a £213 billion savings claim and to mourn Scotland's chances. Its instinct is sceptical but constructive, and its shared conviction, voiced repeatedly this week, is that clinicians and safety officers are not bystanders to the AI rollout but, as one member put it, "the teeth."
APPENDIX A: Detailed Activity Analytics 📊
📬 Total Messages: 454
📈 Peak Day: Thursday 11 June (117 messages)
🔥 Most Active Period: Thursday evening (61 messages)
💬 Average / Active Day: 65 messages
🏖️ Weekend Activity: 12.3% (56/454)
💼 Weekday Activity: 87.7% (398/454)
Daily Message Distribution:
Activity Heatmap by Time of Day:
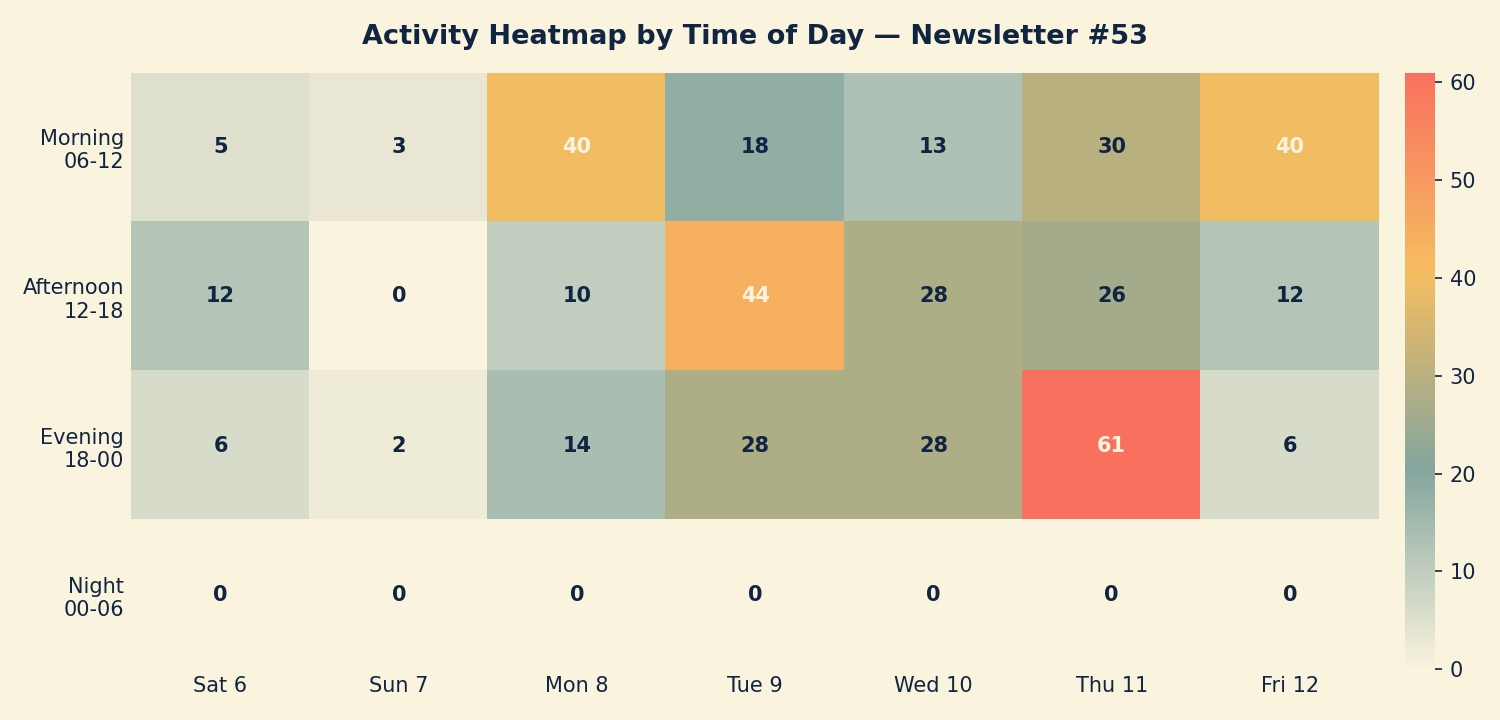
Peak engagement was concentrated in Monday morning (the Copilot announcement), Tuesday afternoon (liability and the Mythos launch) and Thursday evening (the regulation reports, AVT switching and Confed Expo debriefs running in parallel). Activity was overwhelmingly office-hours and weekday, a marked contrast to the typical weekend-heavy pattern, reflecting both the news-driven agenda and the quiet weekend following last week's first-birthday special.
APPENDIX B: Enhanced Statistics
Top 15 Contributors (Role Descriptors Only):
1. Digital Health & Clinical AI Specialist (Group Moderator): 90 messages
2. Integrated care operations lead: 30 messages
3. Tech-literate GP partner: 27 messages
4. Agentic-primary-care GP: 24 messages
5. NHS trust informatician: 21 messages
6. Clinical imaging AI specialist: 21 messages
7. Health tech consultant: 21 messages
8. Hospital innovation lead: 16 messages
9. Radiology AI lead: 15 messages
10. Interoperability specialist: 13 messages
11. GP innovator (Confed drone pilot): 10 messages
12. Edge-AI engineer: 9 messages
13. Medical device regulatory specialist: 8 messages
14. Global digital health specialist: 8 messages
15. Health policy analyst: 7 messages
Hottest Debate Topics:
1. 🔥🔥🔥 AI liability gap and the "beta disclaimer" defence (Tue-Wed, spanning device class, indemnity and MHRA enforcement)
2. 🔥🔥🔥 Copilot for 500,000 NHS staff: savings claims versus clinical reality (Mon)
3. 🔥🔥🔥 Mythos / Fable launch and the US export block (Tue-Sat)
4. 🔥🔥 National Commission and MHRA regulation reports (Wed-Thu)
5. 🔥🔥 Device classification: Class I versus Class II, UKCA versus EU MDR (Wed)
6. 🔥🔥 NHS Confed Expo debrief and the "three holes" critique (Thu-Fri)
7. 🔥 GP2GP, data portability and the supplier duopoly (Thu)
8. 🔥 Local and on-prem models, SAR data and edge AVT (Sat, Wed-Thu)
Discussion Quality Metrics:
• External resource sharing: 59 unique links across the period
• Evidence base: heavy reliance on primary sources, with at least four peer-reviewed papers and seven official policy documents or guidance pages cited
• Constructive challenge: high, with several threads (device classification, GP2GP, Copilot savings) featuring members directly and respectfully disagreeing on evidence
• Distinct contributors: 66
Cross-Expertise Engagement:
The week drew GPs, radiology and imaging specialists, clinical safety officers, interoperability engineers, medicolegal advisers, regulatory and HTA specialists, informaticians and health-policy analysts. The most cross-disciplinary thread was the liability debate, which pulled in clinical, legal, regulatory and product perspectives in a single afternoon. A new chief medical information officer joined and was welcomed during the Copilot discussion.
APPENDIX C: Daily Theme Summary
Saturday, 6 June 2026
Primary Theme: Open, on-prem AVT and edge models Key Discussion: An edge-AI engineer introduced NVIDIA's new streaming ASR model that runs on edge hardware without a GPU, sparking debate on whether commodity edge inference will end profit-making cloud AVT and keep inference out of the USA. Secondary Discussions: Meta ad-trackers and data privacy; an AI hallucinations case study. Notable: Early framing of the open-source and sovereignty theme that would dominate by the following Saturday.
Sunday, 7 June 2026
Primary Theme: Quietest day; newsletter #52 shared Key Discussion: The group moderator shared Issue #52, marking a full year of newsletters, and trailed the first-birthday special edition. Secondary Discussions: a piece on data-firm government contracts; Meta smart-glasses facial recognition. Notable: Just 5 messages, the calm before a busy week.
Monday, 8 June 2026
Primary Theme: Copilot for 500,000 NHS staff Key Discussion: The rollout announcement and savings claims met immediate scepticism, with debate over administrative versus clinical time savings, integration barriers and what "certified as safe" means. Secondary Discussions: HLTH and Confed Expo logistics; Scotland's World Cup and a prediction league; AVT for live translation in consultations. Notable: A new chief medical information officer was welcomed to the group.
Tuesday, 9 June 2026
Primary Theme: The AI liability gap and the Mythos launch Key Discussion: A GPonline article on clinical negligence exposure ran alongside a general question about whether a "beta, for testing only" disclaimer can exempt a therapeutic AI; the group was unanimous that it cannot. Secondary Discussions: Underwater datacentres and heat dissipation; NHS workforce report; the new Anthropic model's arrival to immediate acclaim. Notable: "New Anthropic model alert" landed mid-afternoon and reframed the rest of the week.
Wednesday, 10 June 2026
Primary Theme: Device classification and the regulation reports Key Discussion: A draft NHS framework demanding "Class 2 as a minimum" clashed with the MHRA's apparent Class I trend, opening a detailed debate on UKCA versus EU MDR and CE marking. Secondary Discussions: MHRA enforcement powers and jail-time provisions; Mythos economics and the "token sacrifice" running joke; local models on a 64GB MacBook. Notable: The NHS Shared Business Services framework was revealed to be generic Government AI assurance, not NHS-specific.
Thursday, 11 June 2026
Primary Theme: The National Commission and MHRA reports, plus Confed Expo Key Discussion: The week's busiest day saw the regulation reports condensed into ten findings that mirrored the group's own views, alongside detailed discussion of AVT provider switching, GP2GP data degradation and a critical Confed Expo debrief. Secondary Discussions: SAR for one's own record; the "learned intermediary" history-taking question; the health secretary's call for more risk-taking; "we are the teeth." Notable: 117 messages, 61 of them in the evening.
Friday, 12 June 2026
Primary Theme: Consultancy "AI slop" and the Confed Expo critique Key Discussion: An FT piece on the big four facing AI redundancy launched a long, fond thread on repackaged reports and why the NHS keeps paying for them, while an operations lead set out his "three holes" in the Expo's AI narrative: the cash, the future clinicians and burnout. Secondary Discussions: Frontier models beating clinical AI tools (Nature Medicine); drug-information chatbots and the BNF; police misuse of AI; a creepypasta hospital game. Notable: "We get what we accept. We all have a part to play."
Saturday, 13 June 2026 (to 09:00)
Primary Theme: US export block on Fable and Mythos Key Discussion: News that the US had ordered access suspended for all foreign nationals, including Anthropic's overseas staff, was read as regulatory capture and a fresh argument for sovereign and open-source models. Secondary Discussions: Book recommendations (Empire of AI, Everything is Tuberculosis); an NHS health-data engagement consultation. Notable: Coverage cut-off at 09:00; the export-block thread continued into the next reporting period.
AI in the NHS Weekly Newsletter is produced by Curistica Ltd for members of the AI in the NHS WhatsApp community. All contributors are anonymised. Views expressed are those of individual community members and do not represent any organisation.