Executive Summary
This week the group circled a single, awkward question from several directions: if the real risk in healthcare AI lives in the "last mile" of implementation rather than the model itself, who is actually responsible for it? It opened on the limits of medical device regulation, with the moderator arguing that the overwhelming majority of healthcare technology is not, and will not be, a regulated device, leaving the area of greatest risk uncovered. Skin Analytics' new smartphone clearance became the week's worked example of "doing it properly" over thirteen years, set against a frustration that too much else is open-source algorithms "bolted on and launched". The conversation then turned to the regulator now moving onto this ground: the CQC has named AI as an explicitly assessable topic for general practice, which split the group between those who see overdue accountability and those who fear a tick-box inspection by assessors without the expertise to judge.
The other half of the week was geopolitics and self-reliance. A government review proposing that advanced AI be judged "like doctors", held to clinical standards before taking on clinical work, met broad approval and a sharp aside about suppliers marking their own homework. National-security drama swirled around Anthropic's Mythos and Fable models and a contested claim that one had cracked classified systems, feeding a wider argument that frontier labs are talking up cyber-capability to justify killing off open source. Underneath it ran the group's most practical thread: members running local models on isolated machines, debating whether a GP practice can safely point Claude Cowork at its policy documents, and venting about an NHS that bans password managers while mandating passwords changed every twelve weeks. Add a serious exchange on AI for rare-disease diagnosis, a fellowship the group half-seriously offered to crowdfund, and a Tuesday-night Scotland match, and you have 493 messages across the week. Here are the threads that shaped them.
Activity at a Glance
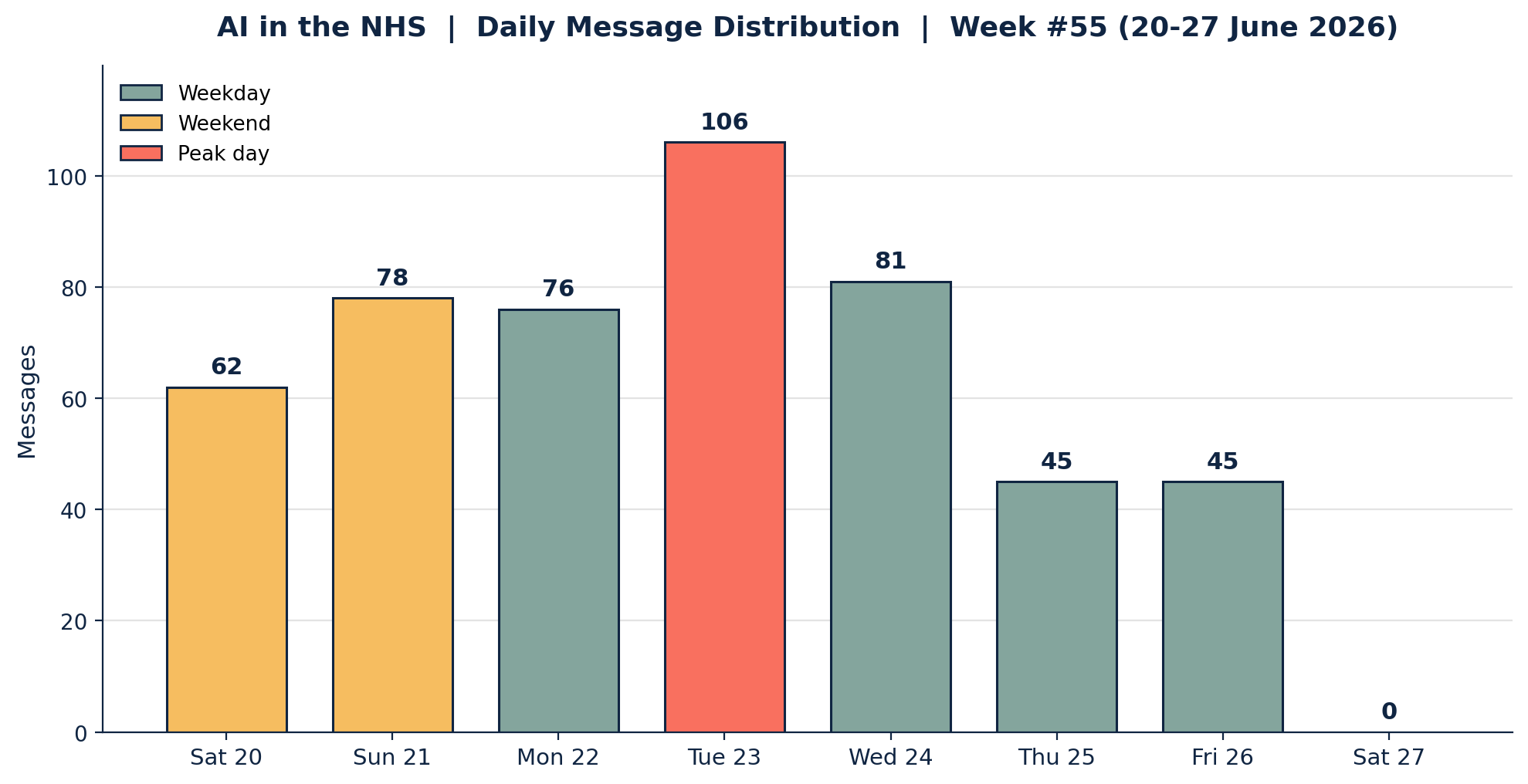
Week 55 generated 493 messages across the seven-day coverage period. Tuesday 23 June was the clear peak (106 messages), its afternoon alone carrying 63 of them across the government review, the Mythos national-security story and a long riff on detecting AI-written text. Sunday 21 June (78) and Monday 22 June (76) were close behind, driven by the AI energy debate and the rare-disease and fellowship threads. Thursday and Friday were the quietest full days (45 each). Weekday traffic dominated at 71.6 per cent, with a livelier-than-usual Saturday and Sunday as the device and regulation discussion got going early.
📌 Major Topic Sections
1. The last mile: devices, DCB standards and the CQC's arrival in AI
Saturday opened on a deceptively simple observation that framed the whole week. Responding to the point that today's AI tools mostly are not medical devices, the moderator argued this is not a loophole that integration will quietly close: "I'd estimate that 80 per cent of the tech involved in healthcare delivery is not (and will not be) a medical device," and his own incident database is "overwhelmingly non-device incidents." Device regulation, he noted, barely touches the implementation-side governance where harm actually occurs, citing the previous year's HSSIB finding that "it is the 'last mile' where the risk lies." His conclusion was blunt: "the area of greatest risk is currently not covered."
That set up the week's standard-bearer for doing it right. News that Skin Analytics had achieved a Class III clearance for use without a dermoscope, on standard smartphone cameras, drew admiration precisely because it was hard-won. An innovation-focused GP pointed out the company has "been working on this tech since 2012, it has taken them nearly 13 years to reach this level, a proper evidence-based approach," in contrast to "a lot of tech, particularly chatbots and some CV applications, just bolting on open-source algos and launching them." An integrated care operations lead made it a principle: "Many AI tech advances are reaching the point that it'd be ethically wrong to not use them," but "standards are everything, and until you have independently verifiable standards for your tool you're just not there." An NHS IT specialist reminded the group that English digital health technologies are already subject to DCB0129 and DCB0160, built on the same ISO 14971 risk-management standard baked into device quality systems, and that even Skin Analytics had survived "cycles of expansion and contraction, including layoffs", a success "despite the odds".
The sharpest exchange came when the regulator entered the frame. The moderator reported that the CQC has signalled a clear direction of travel: under the single assessment framework AI is "named as an explicit, assessable topic area, with innovative use of AI as a possible route to outstanding", and practices should expect "staff training, governance, DPIA, and evidence of procurement diligence" to be "table stakes". Not everyone welcomed it. The innovation-focused GP was "extremely worried if CQC starts to evaluate AI implementation", doubting inspectors have the technical or clinical expertise to judge what is genuinely safe, and predicting "a tick-box exercise: is this tech a medical device, yes/no? DTAC in place, DPIA in place." The operations lead took the opposite view, that many providers would fail even a basic "show me" on their qualifying tech, which "should spark an inadequate without even having to do a quality check", while worrying the new "light touch" inspections are too thin to tell. The moderator landed on the practical question for everyone: what should a non-specialist inspector actually ask, and what can they verify "without resort to SMEs"? His own answer, a technology risk register with every tool and its status, then "lay hands on the artefact", and a reminder that the supply of suitable subject-matter experts cannot be conjured overnight: "decades of under-preparation cannot be undone in a flash."
2. Judge AI like a doctor, and build the people to do it
On Tuesday a government review crystallised the regulation thread into a headline the group liked: "Judge advanced AI systems like doctors." As relayed from the trade press, the commission proposed regulating agentic AI "like human professionals", requiring systems to "demonstrate capability before taking on higher-risk clinical tasks" and telling providers "not to rely solely on monitoring tools introduced by AI manufacturers." The operations lead agreed without hesitation: "If AI wants to replace clinicians then it must be held to at least the same standard as the clinician it replaces. And suppliers marking their own homework is always a stupid idea." A cautious frontline GP found the practical catch immediately: "Getting AI agents to sit written exams is straightforward, and it's testing a skill we know they're good at. How do we get them to sit OSCEs?" A clinical safety advocate supplied the week's most quoted coinage, imagining systems that are "differently trained" yet retain liability for their errors, heralding "the dawn of the AI Associate."
The same energy ran into a concrete way of growing capability inside the NHS. A clinical AI fellowship lead shared a new cohort: two funded days a week for a year to work on a local AI implementation project under supervision, with monthly workshops taught by figures such as Eric Topol, mostly funded through deaneries for those with a training number, though some places are open to anyone in their field. That prompted a genuinely generative discussion about widening access. With the group nearing 800 members, the moderator floated crowdfunding a place, "a tenner each, that's not bad", while a GP federation clinical digital lead and others pressed the more durable idea of PCNs, federations and the RCGP funding fellows tied to local projects. A primary care digital policy lead suggested a briefing session for PCNs and feds considering it, noting the obstacle "is not the cost of the fellowship but the cost of two days' salary." The moderator set out where he would steer a fellow: "advancing clinical risk management in a practical way in primary care for AI", building "a decent primary care benchmark for evals", workforce training, and ways to monitor performance, bias and return on investment, and tied it back to the report's own recommendations as something "this becomes a practical realisation" of.

3. Rare disease, cold cases and the limits of AI diagnosis
Monday's substantive thread asked how far AI can move the needle on diagnosis at the hard end. It began with a report of OpenAI's o3 working through rare-disease cases at Boston Children's, and the obvious question of "when do we get to the point that this is used on undiagnosed cases", of which general practice has many. The data invited caution. A primary care digital policy lead pointed out the study solved 18 of 376 cases, leaving "358 of 376 still unsolved", and that these were curated clinical-genetics puzzles rather than the messy presentations of general practice. A cautious frontline GP added that for every clever pickup there would likely be "many over-investigated common problems that have presented in an atypical way", noting estimates that a fifth of GP consultations never find a cause at all.
Against the scepticism came hard-won enthusiasm. An AI-forward GP described using his own model to take on cold cases that consultants had been unable to crack, and an instance where it untangled a heavily confounded diagnosis of EGPA (formerly Churg-Strauss) previously, and not unreasonably, labelled as fibromyalgia: time to diagnosis two years against an average of seven, "instantly life-changing", and a case he was certain he "could not have solved without AI." His wider claim was that "rare diseases become rare not just because they're one in a million, but because of confounding factors not found in textbooks", a problem that will grow as more patients live longer with multiple conditions. Others reframed the target entirely. The innovation-focused GP argued that "most cases are not rare", and that long diagnostic odysseys usually reflect "poor patient flow management", patients "bounced around between multiple specialties" who cannot see each other's notes, rather than clinicians being stumped; the real value of agents, in his view, is to "automate and serialise the entire non-clinical part of the journey." The moderator offered the unifying frame, that this is "not either-or, it's the additional perspective", and sketched a vision of "a new version of House, where AI-forward clinicians pick up cold cases scouted out by FDP-enabled agents", while reminding the group that "rare diseases are collectively common: one in 17 people are affected by a rare disease at some point in their life."
4. Mythos, distillation and the open-source surge
The week's geopolitical thread tracked the frontier and its discontents. A national-security story about Anthropic's Mythos and Fable models ran alongside a more lurid, member-shared report claiming that "Anthropic's Mythos AI reportedly cracked NSA classified systems in hours", which some read as explaining a recent access ban. The moderator was measured, noting the gap between a red-teaming model and a jailbreak model, and that "national-security agency after agency is now issuing broadly similar assessments", which moved him towards "yep, it's a smart cookie", while flagging that much of the viral coverage was "clickbait" that misrepresented the timeline. An innovation-focused GP was more sceptical still, observing that classified systems are physically separated, that "we really need more technical details", and that the affair looked "politically motivated": in his reading the deeper agenda is that "models are cyber weapons and need FDA-style review before release, all about killing open source to protect trillion-dollar investments." An operations lead reached for history, recalling a 1995 army briefing whose lesson was "if it's connected to the internet, someone will try to break into it", and predicting a return to properly air-gapped systems for anything truly sensitive.
By Thursday the frontier story had curdled into a dispute about who owes what to whom. Anthropic's allegation that Alibaba had "illicitly extracted" Claude's capabilities through distillation drew a wry, evenhanded cynicism rather than partisanship. An innovation-focused GP called it "a bit rich" given the labs' own training practices, and a clinical safety advocate captured the double standard the group enjoyed puncturing: "when WE do it, it's noble and the pursuit of enlightenment; when THEY do it, savage thieves." More than one member concluded that no lab can cleanly claim the moral high ground on intellectual property, with what one called "modern-day pirates" framing applied generously in both directions. The constructive flip side was a quiet confidence in open and local models. The moderator publicly marked his "transformation to the cause" after a performant 3-billion-parameter Baidu OCR model appeared, musing how it would cope with decades of messy handwritten GP notes and noting "a local model doing this would help tremendously with cost and privacy." A digital health strategist supplied the week's manifesto line: "we need to stop waiting for someone else to solve our problems with a shiny new thing, and just make stuff", while an innovation-focused GP declared himself "super confident that we don't need any frontier proprietary labs to deliver true digital productivity."
5. Shadow AI at the coalface: Cowork, isolated Macs and the cyber reality
If the frontier was abstract, the coalface was not. A digital health innovator asked a question many practices are quietly wrestling with: if a GP practice wanted to use a tool like Claude to review and update policy and protocol documents, "nothing containing sensitive or patient data", what compliance applies? The answers mapped the grey zone precisely. A cautious view held that "for any cloud-based tool, I wouldn't feed it anything that you wouldn't be happy to publish to the internet"; others pointed to local models such as Ollama as the safer route, and to the IT-permission and admin-access barriers that make installing such tools on NHS machines unlikely. The most useful contributions were operational. A practice-based digital lead described running "Claude Cowork at the moment, in the testing phase", on a Mac "not connected to any NHS anything", strictly for already-public operational policies: "a complaints policy yes; thematic responses on complaints, absolutely not." A practice manager described the same pattern, doing "any AI wrangling outside of the NHS network so the IT team don't get the collywobbles", via an off-site machine fed by email and dispatch. The shared conclusion was that the work is less about the tool than about "doing a good assessment, having a framework of what is okay to share, and a clear process for doing it."
Wednesday turned the same lens on NHS cyber-security, with predictable exasperation. An innovation-focused GP named "having a billion passwords that each need to be changed every 12 weeks" as "one of the biggest cyber risks in the NHS", made worse because "password managers are not allowed." An NHS IT specialist agreed the prohibition was baffling against current best practice of single sign-on, a complex password that rarely changes, and MFA, while noting how few trusts use the central NHS identity platform for anything beyond email. The operations lead located the root cause in chronic under-investment, recalling a £234-per-person annual training budget on joining the NHS in 2014, proudly described as "NHS leading", against the £2,000-plus he was used to in the private sector, and a typical NHS information-security manager being "a rebadge or sideways promotion with zero effective training at that grade." A welcome corrective arrived from a member close to the standards: the updated DSPT aligns to the NCSC's framework, "password managers using MFA are actively encouraged, four-digit PINs are discouraged", and the shift is towards "three random words", so the blanket bans some members face are local interpretation rather than national policy. The same instinct for lightweight, public-good tooling surfaced in admiration for a shared tool comparing NHS waiting times by postcode, praised for using public data and a privacy-forward design, even as it exposed how poor the underlying data can be: one member reported a local hospital "advertising waits of 18 weeks, but for the past 12 months patients being told it is 48." As the moderator put it, fixing this is "like squeezing bubbles out of a screen protector, you nail one and another pops up", but the pressure it applies to source-data quality is no bad thing.
😄 Lighter Moments
For all the regulation and geopolitics, the group kept its sense of humour firmly intact. Tuesday night delivered the inevitable football saga as Scotland faced Brazil at the World Cup, complete with members feeding the match into Claude for predictions and finding its optimism unconvincing: "an 85 per cent chance of progression isn't enough for me, need more promising data." When one member assumed the moderator's frequently-cited brother "Dougal" must be an AI, he was reassured that Dougal is one of five real brothers, "some name for an AI". The verdicts grew fonder as the score worsened, from "VAR has better defence than Scotland" to a plea to sub off the centre-backs, and a mock-heroic invocation of "Shuftie McVar of the Clan McVar, born in 1518 on the shores of Loch Shiel, and our hope is immortal." The Onion obliged with a piece on Scottish fans that the group wore as a badge of honour.
Elsewhere the personality showed in the asides. A solstice reminder to "practise safe sun" arrived attached to an alarming wellness blog about a sunbathing practice best left undescribed. A long, self-aware thread on detecting AI-written text produced the week's koan, "if you can't tell what's AI or human-generated, and the AI can't tell either, are we even awake?", and a rueful confession that everyone's vocabulary is now "scattered with 'stale', 'load-bearing', 'honest' and other literary equivalents of em-dashes." One member's heartfelt substack about rehabilitating a traumatised dog was unhelpfully flagged as AI-generated by a detector, prompting the deadpan note that "as a former soldier, quite likely I'd have eaten the crayons." And Friday's discovery that pigeons can be trained to spot abnormalities on CT scans sent the group down a delightful rabbit hole, from Project Pigeon to RFC 1149, the 1990 standard for carrier-pigeon internet, offered in all seriousness as a sovereignty-proof transport layer after the moderator's own flight was delayed by a bird strike.
💬 Quote Wall
"The area of greatest risk is currently not covered." — The group moderator, on the implementation 'last mile' beyond device regulation
"Standards are everything, and until you have independently verifiable standards for your tool you're just not there." — An integrated care operations lead
"If AI wants to replace clinicians then it must be held to at least the same standard as the clinician it replaces. And suppliers marking their own homework is always a stupid idea." — On the government review proposing AI be judged like doctors
"Replace them with 'differently trained' agents but make them retain liability for the errors. We herald the new dawn: the dawn of the AI Associate." — A clinical safety and governance advocate
"Rare diseases become rare not just because they're one in a million, but because of confounding factors not found in textbooks." — An AI-forward GP, on diagnostic odysseys
"We need to stop waiting for someone else to solve our problems with a shiny new thing, and just make stuff." — A digital health strategist, on open source
"When WE do it, it's noble and the pursuit of enlightenment. When THEY do it, savage thieves." — A clinical safety advocate, on the distillation wars
"Any AI wrangling outside of the NHS network, so the IT team don't get the collywobbles." — A practice manager, on running AI from an off-site machine
📎 Journal Watch
Academic Papers and Key Studies
📎 Perspective on digital health technologies and medical device regulation – npj Digital Medicine. Shared with a pointed "Yet..." into Saturday's debate about whether AI integrations will, or should, drag more healthcare software into device regulation. Read more
📎 Pigeons as trainable observers of pathology – PMC. A 2015 study resurfaced when news broke that pigeons can spot abnormalities on CT, evidence that avian pattern-recognition is a serious, if unlikely, line of research. Read more
📎 The temporarily dependent patient in general practice – PubMed (K B Thomas). A 1970s classic invoked in the rare-disease thread as a reminder that much of what presents has no findable cause, and that uncertainty management is core GP work. Read more
📎 Making sense together after algorithms – BJGP Life. A reflective piece on sense-making in primary care once algorithms enter the consultation, shared into the diagnosis discussion. Read more
📎 BMC Primary Care: call for papers – Springer. A collection guest-edited within the group's wider network, circulated as an invitation to contribute primary care AI research. Read more
Industry and News Articles
📎 Judge advanced AI systems like doctors, says government review – HSJ. The week's pivotal policy story: a commission proposing agentic AI be regulated like human professionals, demonstrate capability before higher-risk clinical work, and not be monitored solely by its own makers' tools. Read more
📎 Anthropic, Claude, Fable and national security – The Guardian. Context for the Mythos and Fable national-security thread that ran through Tuesday. Read more
📎 Anthropic says Alibaba illicitly extracted Claude capabilities – Reuters, with companion coverage in Ars Technica. The distillation dispute behind Thursday and Friday's argument over who really owns model capability. Read more Read more
📎 Digital medical device for cancer detection certified for smartphone use – Med-Tech Insights. The Skin Analytics smartphone clearance that anchored the "doing it properly" discussion. Read more
📎 Something's off with Midjourney's pivot to body scanners – The Verge. A sceptical write-up of the image-generator's medical move, judged "unserious until they do something medical with it." Read more
📎 Pigeons excel at spotting abnormalities on CT scans – Radiology Business. The "not satire" article that launched Friday's pigeon thread. Read more
📎 AI is everywhere in medicine, so why aren't students being trained to use it? – Medscape. Prompted a short exchange on what an AI curriculum's priorities should be, "starting with general principles" that will keep changing. Read more
📎 Compare NHS waiting times by hospital and postcode – LinkedIn (shared tool). A lightweight, privacy-forward tool praised as an example of turning hard-to-navigate public data into something genuinely useful for patients. Read more
Technical Resources and Commentary
📎 A cheat sheet for conversations about AI's energy and water use – Andy Masley. The detailed, sourced post behind Sunday's energy debate, credited with changing some minds on per-prompt water and energy costs. Read more
📎 The vibe-coding spectrum: AI-assisted software development – NCSC. Shared into the recurring worry about security risks when non-engineers ship AI-generated code. Read more
📎 The AI shift in cyber risk: why leaders must act now – NCSC. Read by some as stating the obvious, but a useful anchor for the cyber-leadership and connected-device thread. Read more
📎 GLM 5.2 – Simon Willison. The write-up behind the week's open-model enthusiasm and the running joke about running it locally on a "mainframe". Read more
📎 Baidu Unlimited-OCR (3B) – Hugging Face. The performant open-source OCR model that prompted the moderator's public "transformation to the cause" of local models, and the question of how it copes with decades-old handwritten GP notes. Read more
📎 Vaultwarden – GitHub. A self-hosted, open-source password manager offered as a practical answer to the NHS password-manager ban. Read more
📎 Using AI for thematic analysis of coroner reports – Wolfram Blog. A worked precedent for Thursday's idea of mining Prevention of Future Deaths reports for technology-related harms, potentially paired with MHRA Yellow Card data. Read more
📎 Preventable Deaths Tracker – preventabledeathstracker.net. Surfaced as an existing resource for analysing coroners' Prevention of Future Deaths reports at scale. Read more
📎 Medical Event Data Standard (MEDS) – MEDS docs. Shared with a clinical-modelling caution about losing the context that makes AI "really sing", even where the standard is intended for training rather than records. Read more
Policy Documents and Official Reports
📎 GP Mythbuster 109: artificial intelligence in GP services – CQC. The regulator's own guidance, central to the week's debate about how AI will be inspected in general practice. Read more
📎 Guidance on protecting connected medical devices – NHS Digital. Cited against the "just accelerate patching" advice, which can be impossible for connected medical devices, with better-targeted mitigations set out here. Read more
📎 Prevention of Future Deaths reports – Courts and Tribunals Judiciary. The primary source behind the coroner-reports analysis idea, a searchable archive of PFD reports. Read more
📎 What is a rare condition? Rare condition registration statistics – NHS Digital. The source for the "one in 17" figure that reframed rare disease as collectively common. Read more
🔭 Looking Ahead
The regulation thread will run on. The CQC's move to make AI an explicitly assessable topic in general practice means staff training, governance, DPIAs and procurement-diligence evidence are becoming "table stakes", and the group will keep working out what a meaningful, non-specialist inspection actually looks like. The government review proposing that AI be judged to clinical standards is likely to draw sustained input. On the workforce, expect follow-up on whether PCNs, federations or the RCGP can fund clinical AI fellowships tied to local projects, with a briefing session for interested organisations floated. The moderator is keynoting the Isle of Man Innovation Challenge 2026 finale, streamed, with the group earning a name-check. The sovereignty and open-source conversation continues as members watch the Anthropic and Alibaba distillation dispute, the staggered release of the next frontier models, and the steady maturing of local options such as GLM 5.2 and open OCR. And several members are circling a concrete build: an agentic, human-in-the-loop layer for Advice and Guidance triage, "free text plus an attachment, basically a chatbot interface", with at least one NIHR-funded team already reported to be working in the space.
🧬 Group Personality Snapshot
This is a community that treats a Class III device clearance, a carrier-pigeon RFC and a Scotland World Cup capitulation with exactly the same blend of rigour and mischief. It is sceptical of frontier-lab theatre yet quietly busy with the practical alternative, running quantised models on isolated Macs, swapping self-hosted password managers, admiring a postcode-level waiting-times tool built over a weekend. Its instinct is to ask who is actually accountable when something goes wrong, and to prize "independently verifiable standards" over marketing, while staying generous with hard-won experience, whether that is a single rescued diagnosis after a two-year odyssey or a frank account of an NHS training budget of £234 a head. It reads the regulator's guidance line by line, argues about distillation ethics with evenhanded cynicism, offers to crowdfund a colleague's fellowship, and still finds time to christen an imaginary VAR official of the Clan McVar. Above all it keeps returning to the same test: not what AI can do, but what it does for patients, for frontline workload, and for the last mile where the real risk lives.
APPENDIX A: Detailed Activity Analytics 📊
📬 Total Messages: 493
📈 Peak Day: Tuesday 23 June (106 messages)
🔥 Most Active Period: Tuesday afternoon (63 messages)
💬 Average / Active Day: 70 messages
🏖️ Weekend Activity: 28.4% (140/493)
💼 Weekday Activity: 71.6% (353/493)
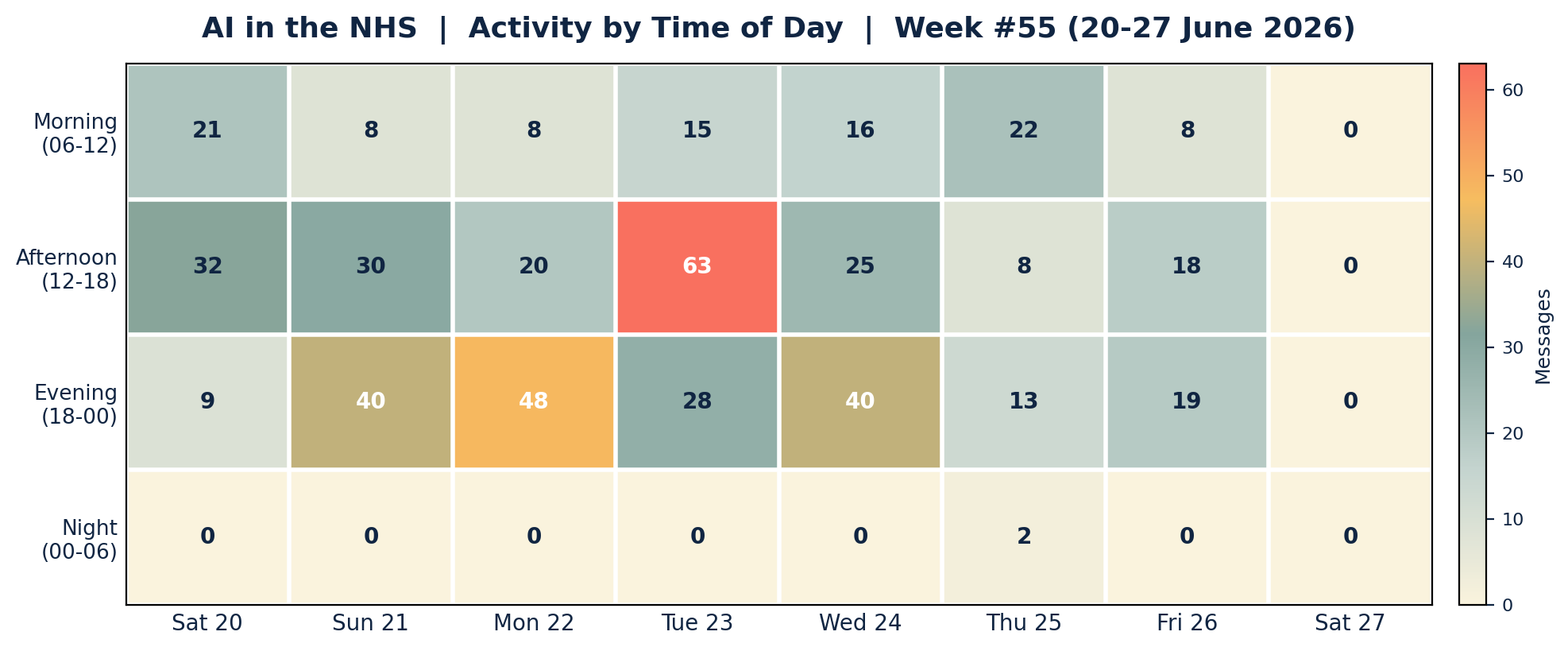
Engagement clustered in the afternoons and evenings, with Tuesday afternoon the single busiest window (63 messages) around the government review and the Mythos national-security story. Sunday and Monday evenings were the other hotspots, carrying the AI energy debate and the rare-disease and fellowship threads. Mornings were steadier than usual as the device and CQC discussion got going early on Saturday. Night-time activity was almost nil, a single pair of messages in the small hours of Thursday after the late Scotland match.
APPENDIX B: Enhanced Statistics
Unique Contributors: 63 group members posted at least one message this week, out of the group's wider membership of nearly 800. The 15 most active below account for 363 of the 493 messages (73.6 per cent), with a long tail of occasional and one-off contributors making up the remaining 130 messages.
Top 15 Contributors (Role Descriptors Only):
1. Digital Health & Clinical AI Specialist (Group Moderator): 119 messages
2. Integrated care operations lead: 32 messages
3. Innovation-focused GP: 32 messages
4. Clinical safety and governance advocate: 29 messages
5. Digital health GP exploring local models: 21 messages
6. GP and frequent blogger: 20 messages
7. Digital health technologist: 18 messages
8. NHS IT specialist (former utilities sector): 14 messages
9. GP federation clinical digital lead: 14 messages
10. Primary care digital policy lead: 13 messages
11. Digital health contributor: 13 messages
12. Digital health innovator: 10 messages
13. GP interested in AI diagnostics: 10 messages
14. Practice-based digital lead: 10 messages
15. Academic primary care researcher: 8 messages
Hottest Debate Topics:
1. 🔥🔥🔥 The last mile, devices, DCB standards and CQC's move into AI (Sat)
2. 🔥🔥🔥 Mythos, national security and the distillation wars (Tue-Fri)
3. 🔥🔥 Shadow AI for practice admin, isolated Macs and the NHS cyber reality (Sun, Wed)
4. 🔥🔥 Judge AI like a doctor, and the clinical AI fellowship (Tue, Mon)
5. 🔥🔥 Rare disease, cold cases and the limits of AI diagnosis (Mon)
6. 🔥 AI energy and water costs, training externalities and what-aboutism (Sun)
7. 🔥 Detecting AI-written text, GPTZero false positives and "AI slop" (Tue)
8. 🔥 Coroner reports, Yellow Card data and technology-related harm (Thu)
Discussion Quality Metrics:
• External resource sharing: more than 40 unique links across the period, spanning peer-reviewed papers, official guidance, trade press and open-source tooling
• Evidence base: strong, with an npj Digital Medicine perspective, NHS Digital statistics, NCSC and CQC guidance and a 1970s general-practice classic all cited directly
• Constructive challenge: high, with the rare-disease, CQC-inspection and energy-cost threads featuring sustained, respectful disagreement grounded in data and lived experience
• Breadth of participation: 63 unique contributors, with the moderator aside no single voice exceeding 6.5 per cent of total volume, a well-distributed week
Cross-Expertise Engagement:
The week drew GPs and GP partners, practice managers, radiology and hospital voices, NHS IT and information-security specialists, informaticians and data-standards experts, operations and federation leads, health-tech founders and developers, medical educators and academic researchers, and clinical-safety and policy leads. The most cross-disciplinary thread was Saturday's device-and-CQC debate, which pulled regulatory, clinical, operational, commercial and inspection perspectives together. New members were welcomed during the week, including a former medical-imaging company chief executive.
APPENDIX C: Daily Theme Summary
Saturday, 20 June 2026 (from 09:00)
Primary Theme: The 'last mile', medical devices and the CQC moving onto AI Key Discussion: A debate that most healthcare tech is not, and will not be, a regulated device, leaving implementation risk uncovered, set against Skin Analytics' smartphone clearance as the model of doing it properly, and the CQC naming AI as an explicitly assessable topic for general practice. Secondary Discussions: DCB0129/0160 and ISO 14971; whether "light touch" inspections can judge AI; DPIA responsibility in procurement; vibe-coding security; wearables and online-consultation demand. Notable: The week's defining question, who owns the last-mile risk, was set on day one.
Sunday, 21 June 2026
Primary Theme: AI energy and water costs, and the open-source case Key Discussion: A detailed, sourced cheat sheet on per-prompt energy and water use changed some minds, while members debated whether training and rare-earth externalities belong in the sum, and whether the same scrutiny is applied to anything else we consume. Secondary Discussions: Open source versus proprietary economics; using Claude Cowork or local models for GP practice policy admin; Copilot availability for GP surgeries; NotebookLM for long reads. Notable: Newsletter #54 went out to the group and mailing list on the solstice.
Monday, 22 June 2026
Primary Theme: Rare disease, cold cases and the limits of AI diagnosis Key Discussion: An OpenAI o3 rare-disease report (18 of 376 cases solved) split the group between scepticism about value in general practice and hard-won enthusiasm, including a rescued EGPA diagnosis, with a counter-argument that long odysseys reflect poor patient flow more than clinician failure. Secondary Discussions: The NHS clinical AI fellowship and how to widen access via PCNs, federations and the RCGP; crowdfunding a place; redesigning the non-clinical patient journey with agents. Notable: "Rare diseases are collectively common: one in 17 people."
Tuesday, 23 June 2026
Primary Theme: Judge AI like a doctor, and the Mythos national-security story Key Discussion: A government review proposing agentic AI be regulated like human professionals met broad approval and the "AI Associate" coinage, while a contested report that Mythos cracked classified systems fed a wider argument about cyber-capability claims and killing open source. Secondary Discussions: Detecting AI-written text, GPTZero false positives and "AI slop"; Midjourney's body-scanner pivot; the NHS pension and Capita; a Japanese swarming-agents model; Claude tag. Notable: The busiest day of the week (106 messages), 63 of them on Tuesday afternoon alone.
Wednesday, 24 June 2026
Primary Theme: NHS cyber reality, passwords and lightweight public-good tools Key Discussion: Frustration that password managers are banned while passwords must change every 12 weeks, corrected by a member noting the DSPT actively encourages MFA password managers and "three random words", alongside admiration for a member-built NHS waiting-times-by-postcode tool and the poor source data it exposed. Secondary Discussions: Under-investment in NHS IT and information security; a Baidu open-source OCR model and local models for decades-old handwritten GP notes; a first TPP SystmOne to Medicus practice migration. Notable: The late-night Scotland versus Brazil match took over the evening.
Thursday, 25 June 2026
Primary Theme: Distillation ethics and open-model confidence Key Discussion: Anthropic's allegation that Alibaba distilled Claude's capabilities drew evenhanded cynicism about who really owns model capability, alongside growing confidence that open and local models can deliver real productivity without frontier proprietary labs. Secondary Discussions: Mining coroner reports and Yellow Card data for technology-related harm; the Medical Event Data Standard and loss of context; training medical students to use AI; a federation's agentic primary care kick-off. Notable: A half-serious suggestion to spin off a separate group for non-NHS AI chatter.
Friday, 26 June 2026
Primary Theme: Pigeons, open source and automating Advice and Guidance Key Discussion: A genuine study on pigeons spotting CT abnormalities sent the group from Project Pigeon to RFC 1149, while a serious strand argued for an agentic, human-in-the-loop layer over Advice and Guidance triage, "basically a chatbot interface", and noted an NIHR-funded team already in the space. Secondary Discussions: The Anthropic and Alibaba dispute continued; the staggered release of the next frontier models; the Isle of Man Innovation Challenge; tax, avoidance and a 1920s Scottish judge. Notable: The moderator was fogbound on the Isle of Man, musing on pigeon post as a sovereignty-proof transport layer.
Saturday, 27 June 2026 (to 09:00)
Primary Theme: Quiet handover Key Discussion: No in-window human messages before the 09:00 cut-off; the week's threads carried into the next reporting period. Secondary Discussions: None. Notable: Coverage closes at 09:00 on Saturday 27 June.
AI in the NHS Weekly Newsletter is produced by Curistica Ltd for members of the AI in the NHS WhatsApp community. All contributors are anonymised. Views expressed are those of individual community members and do not represent any organisation.