Executive Summary
This week the group lived inside the aftermath of the US export block on Anthropic's Fable and Mythos models, and the mood hardened from shock into strategy. What had been an abstract preference for open source became an urgent, practical question of sovereignty: whether the UK should build its own frontier model, whether a middle-power collaboration is the realistic route, and how far a rush to Chinese open models and on-prem inference can carry primary care that cannot afford to rely on shifting sands. By Wednesday the group had turned to something more concrete and more its own: a forensic debate on ambient voice technology, prompted by a supplier warranting only "97 per cent accuracy," that ran through human error baselines, whether raw consultation audio should be retained like radiology images, and the storage bill the NHS could never stomach.
Friday was the biggest day of the week by far, 170 messages, and it turned existential. A patient who believed an AI had diagnosed their ADHD set off a long, candid argument about clinical de-skilling, referral inflation among AI-reliant trainees, and whether general practice is sliding towards a two-tier, subscription future. That flowed into an unusually personal exchange on GLP-1 weight-loss drugs, the case for letting NHS GPs charge for evidence-based care, and a shared frustration that none of the week's innovation is deliverable under the current GMS contract. Around the heavy themes ran Midjourney's startling pivot into medical body-scanning, a week of HLTH Europe in Amsterdam, and the group's reliable gallows humour about Scotland, England and a neural network built out of goats. Five hundred and seventy-seven messages across seven days; here are the threads that shaped them.
Activity at a Glance
Week 54 generated 577 messages across the seven-day coverage period. Friday 19 June was the clear peak (170 messages), an all-day marathon on de-skilling, the two-tier future and GLP-1 reform, with morning and afternoon almost equally busy. Wednesday 17 June was the second spike (115 messages) around AVT audio retention and the sovereignty debate. Monday 15 June was the quietest full day (18 messages). Weekday traffic dominated at 74.5 per cent, though the weekend bookends were livelier than last week as the export-block fallout ran hot.
📌 Major Topic Sections
1. After the export block: sovereignty stops being hypothetical
The week opened in the long shadow of the previous Saturday's news that the US had ordered Anthropic to disable Fable and Mythos for foreign nationals. Where last week the reaction was disbelief, this week it was planning. A digital health strategist offered three observations that framed much of what followed: that a lab which spends "every interview crying wolf about how dangerous your model is" should not be surprised when "the village finally responds" with regulatory capture; that a wave of AI IPOs could "suck unheard of cash out the system," leaving other countries unable to close the inference gap; and that "owning your own inference has never been more important, no one can build a successful business on shifting sands."
Over the weekend the group moderator posted a deliberately balanced reconstruction of the standoff, contrasting the US government line, that a trusted partner had demonstrated a real jailbreak and Anthropic had refused to fix or pull the model, with Anthropic's position that the jailbreak was narrow, that perfect resistance is impossible, and that the same technique works on other frontier models not subject to the controls. His own conclusion marked a shift: having previously argued against a UK sovereign frontier model on cost grounds, he now thought "it's needed regardless," or failing that "a middle power collab, eg EU, Canada." Others were more sceptical that talk would become action, one member noting that the UK and EU remain "stuck in a regulation mindset" when "we need viable alternatives," and that sovereignty was "all talk."
By midweek the framing had sharpened into national strategy. A widely shared Fortune piece on the "global scramble for sovereign AI" prompted the observation that "the UK is looking very alone on these matters," with the wry forecast of "here's your bill and conditions to rejoin the EU." The moderator took aim at domestic friction, calling resistance to homegrown efforts such as Cogstack and Foresight the AI equivalent of NIMBYism: "Do we want sovereign AI or not? It comes with costs." An operations lead tied it to a longer national story of "build-nothing mode," from nuclear plants to steel, and a political class unwilling "to think beyond the next general election."
2. The open-source answer, in practice
If sovereignty was the strategy, open and local models were the tactics, and this was the week the group put them to work. A new open release, GLM 5.2, circulated under the half-joking banner of "the open model nobody can ban," with members swapping notes on running it through LM Studio, llama.cpp and 2-bit quantised builds. The moderator reported MedGemma 4B and 27B "running locally now (quantised)" and "pretty nippy"; another member was running Qwen and MiniMax on his own machine, and noted that with the new mobile operating system you can now "choose alternates to Apple's own AI model."
The backdrop was a striking shift in the global pecking order. One member relayed data showing Chinese systems as the five most popular models on a major routing platform in the past week, where "a year ago, the five top models were all American," summarising the strategy as one China has used "in everything from furniture to electric cars: it does not have to be the best but it can be the cheapest." The verdict from a GP running his own AI stack was blunt: when open models match frontier performance "in 95 per cent of cases, it makes no logical sense to use anything other than open source."
A realist counter-current ran underneath the enthusiasm. Several members argued the differentiator is no longer the model. "They're all RAG with different source bases," one put it, "different flavours of the same ice cream," and another located the real problem precisely: "The gap isn't in RAG. The gap lies in medicolegal defensibility." An NHS IT specialist added a note of healthy suspicion that "a portion of what passes for 'agentic' AI is just rules-based engines acting deterministically on AI model outputs," a reminder that the group prizes plumbing over branding.

3. Keeping the audio: AVT accuracy and the storage you cannot afford
Wednesday produced the most characteristically rigorous thread of the week, sparked by an operations lead reading an ambient voice supplier's service level agreement that warranted "greater than 97 per cent accuracy," defined as transcripts that "don't contain hallucinations or clinically relevant omissions." Is 97 per cent acceptable, he asked, "or are those two providers just low outliers?" The moderator reframed the question that matters: "how accurate are the human notes against which they are being compared, and what category of errors?"
The human baseline turned out to be sobering. The moderator recalled an out-of-hours audit years ago suggesting around 10 per cent of human notes had minor errors and 5 per cent or fewer carried major omissions. A clinician-founder cited his own small studies putting the human hallucination rate "approx 7 per cent and omission rate around 10 per cent, which is far far below AVT standards now," and "definitely worse in hospitals." That set up the real fight, over whether raw audio should be retained at all. One GP argued it should be kept as long as any other record, just as radiology images and histology slides are, reporting "one objection of the 2000-plus" patients in his explicit-consent, local-stack service. An academic GP pushed back on acceptability rather than feasibility: "my patients would riot," citing a reasonable expectation of privacy and low institutional trust in his part of south-east London, where even a quarter of patients once declined recording for exam revision.
The economics closed the argument down. With around 400 million consultations a year, even recording a tenth of them would run past a petabyte annually before backup, search, information governance and security costs, prompting jokes that the NHS would inevitably "choose FLAC, just like it uses TIFF." A 30-day retention window emerged as the pragmatic compromise, with one practice reporting it wipes audio and transcript every 24 hours, and a recurring worry about the subject access request burden if everything were kept. As one member summed up the group's instinct: "we need to stop being selective in our championing of the principles."
4. De-skilling, referrals and the two-tier future
Friday's marathon began with a quiet anecdote: a patient arrived having seen a counsellor whose AI had "listened in" and suggested an ADHD assessment, and "the patient thought the AI was making the diagnosis." That opened the week's rawest debate. A GP educator reported a referral audit in which a supervisor referred 20 per cent of patients while his AI-reliant trainee referred 70 per cent, warning that AI "offers certainty" to a profession already drifting from generalist risk-management towards protocol-driven pathways. His core message: a doctor focused on "transactional care, without being able to manage uncertainty," should "prepare to be replaced."
An AI-forward GP who has built his own deprescribing tool argued the opposite trajectory for those who use AI well, that he now refers far less because he no longer needs to escalate every edge case, and offered the line of the week: "AI will make bad doctors worse. AI will make good doctors into great doctors. AI will make great doctors into oracles." An operations lead was harsher on those who lean on it without the experience to check it: "if AI does most of your job for you, you're 90 per cent redundant already." But he was equally clear about where unchecked progress leads, refusing to accept a future of private "subscription" doctors for those who can pay: "I didn't join the NHS to just give good care to the 'haves'."
The futures on offer ranged from the dystopian to the defiant. One member predicted "every patient who can afford one will have their own private doctor," with a "K-shaped drift happening in real time"; another sketched a "Ready Player One" world of a few clinical "communicators" providing the human layer over AI-run consultations, even walk-in "photo booth" health checks. Against it, a GP marshalled the Commonwealth Fund's ranking of the NHS as among the best systems in the world and Muir Gray's definition of the clinician's job as helping "that lonely, anxious individual" make the right decision for them. A frontline GP captured the daily reality underneath the theory: complaints "clearly written by AI," patients arriving with ChatGPT-generated test demands, and a system "preparing for yesterday's war, not tomorrow's." The moderator's framing held the tension without resolving it: "the NHS will exist as long as people believe in it, and faith is waning," while "people have a right to seek care from where they choose," and "managing what this means for equity is not at all easy, and cannot be perfectly solved."
5. Plan B for general practice: GLP-1s, McPrescribers and charging patients
The two-tier debate flowed naturally into the week's most personal thread. A frontline GP argued that the profession's real "Plan B" should be the freedom "to charge our patients for certain evidence based non-GMS investigations and treatments. No snake oil," pointing to the absurdity of patients paying online "McPharmacies" £200 or more a month for weight-loss drugs and then coming to their GP, for free, to manage the side effects. The health economics were laid out plainly: roughly £12 billion a year on type 2 diabetes, a reported £95 manufacturer-to-NHS price that would still save money over a lifetime of obesity-related conditions, and eligibility rules that force patients to accumulate "4 or 5 obesity related conditions," most of them in their eighties, before they qualify.
What lifted the thread was the candour. Two members shared detailed personal results from GLP-1 treatment, one reporting a 30kg loss with total cholesterol of 2.9, an HbA1c falling from pre-diabetic into the normal range and liver function normalising, the other 34kg in eight months with an HbA1c of 22. Both described the same revelation, the disappearance of "food noise" they had not realised was there, after decades of restrictive diets that left them "miserable every waking moment." It prompted a half-serious proposal for an "AI in the NHS weight loss challenge" and a broader point about where AI fits: as a lifestyle companion and coach for the part of the pathway, behaviour change, that the McPrescribers treat as "a bothersome nuisance." The reform message was consistent throughout: give general practice meaningful income streams and "breathing room to innovate," and the same GPs would stop seeing AI as a threat of pure workload generation.
6. Midjourney's medical pivot and the wellness-scan hype
The week's most-shared curiosity was a pivot almost too strange to credit: Midjourney, the AI image-generation company, launched a "medical" arm claiming an ultrasound-based machine that scans the whole body in about 60 seconds at "MRI-level resolution," which it said was 100 times faster and 10 times cheaper than MRI. The group's scepticism was immediate and entertaining. One member nailed his colours "to the mast saying it's BS"; another invoked nominative determinism, predicting the company would "exit or fold in the same number of years since they founded"; and a trade-press write-up describing a "medical spa where patients bathe in golden light" did little to help. Members noted an existing service already offers full-body scanning for a few hundred pounds, and raised the perennial spectre of incidental findings sending well patients down "an unnecessary MRI, ad infinitum."
The balanced verdict came from a clinician-founder: "who knows if whole body ultrasound is a good idea, that's what science is for. When they do their FDA and clinical trials in 5 years we will know. If they don't, it's just some silly noises." It was a fitting motif for a week spent at HLTH Europe in Amsterdam, where several members gathered for a group photo, a vendor launched a "complete medical assistant" billed as Class IIa, and, in one surreal aside, an exhibitor was reportedly asked to leave the floor. As one member observed of the wider trend, "the AI pivots are my favourite thing about this timeline."
😄 Lighter Moments
For all the existential weight, the group kept its footing in humour. A week at HLTH Europe produced a steady stream of Amsterdam dispatches, booth logistics and the search for the giant Union Jack "in the sky" to orientate the group photo. The football provided the usual emotional rollercoaster, from Scotland's familiar fortunes to genuine surprise that England were "actually playing amazing football," tempered instantly by the question of "when do they get knocked out on penalties by Germany?" and the firm reply, "never again, never again."
The week's best operational saga came from a practice-based GP and digital lead whose IT team, having noticed his computer's processor running at 100 per cent for ten hours a day, proposed to fix the problem by shrinking his hard drive so he could no longer analyse data, a move he met with weary expertise. The same thread surfaced a 92-inch touchscreen TV delivered to a practice, too heavy for the wall, used for about three hours before disposal, "aka £2,000 per hour," and a box of pulse oximeters nobody asked for. Elsewhere, a member shared news of a Microsoft researcher who built "a working neural network out of goats in Age of Empires II" to critique AI science, the 3D-printing enthusiasts compared notes (including German pharmacists reportedly printing their own medicines), and a long-running gag about Copilot being "basically just Clippy for the new generation" rubbed along with a heartfelt "I HAVE SEEN THE LIGHT" from a new convert to local models.
💬 Quote Wall
"AI will make bad doctors worse. AI will make good doctors into great doctors. AI will make great doctors into oracles." — An AI-forward GP, on the coming divergence in outcomes
"Owning your own inference has never been more important. No one can build a successful business on shifting sands." — A digital health strategist, on the export block
"The gap isn't in RAG. The gap lies in medicolegal defensibility." — A clinician-technologist, on what actually separates clinical AI products
"The NHS will exist as long as people believe in it, and faith is waning. For the believers working in it, our job is to give people good reason to feel the same." — The group moderator
"We're preparing for yesterday's war, not tomorrow's." — A frontline GP, borrowing a line on Defence for the NHS
"It does not have to be the best, but it can be the cheapest." — On China's open-model strategy
"A solid majority of the returns and reports we have to generate in the NHS are shamefully stupid and could be deleted without notice." — An integrated care operations lead
"Who knows if whole body ultrasound is a good idea, that's what science is for." — A clinician-founder, on the Midjourney medical pivot
📎 Journal Watch
Academic Papers and Key Studies
📎 Mirror, Mirror 2024 – Commonwealth Fund. Cited in the two-tier debate as evidence that the NHS model still ranks among the best-performing health systems internationally, and that "private means someone profits" rather than necessarily delivering efficiency. Read more
📎 Nature research paper on AI agents – Nature. Shared into Friday's late discussion on agentic AI, alongside the week's running theme that management skill, not model choice, determines whether agents succeed. Read more
📎 Nature research paper (s41586-026-10764-5) – Nature. Flagged on Thursday as "very interesting" during the local-models and agents exchange. Read more
📎 A general-purpose model across medicine, coding and navigation – Nature. A Nature news article shared on Thursday, noted for spanning clinical, coding and navigation tasks in a single system. Read more
📎 Patient experience and trust in NHS primary care – South West London ICS. Offered as evidence that institutional trust varies sharply by area, central to the argument about whether retaining consultation audio is acceptable to patients. Read more
Policy Documents and Official Reports
📎 MHRA invites views on proposed changes to medical device regulation – gov.uk. The week's key open consultation, landing into the running classification debate and the sovereignty discussion. Read more
📎 NHS workforce plan "based on false assumptions," unions warn – GPonline. The Saturday article that opened the week, criticised in the group as a plan that takes "staffing problems, add AI, and they'll all be fine." Read more
📎 National AI strategy for Canada – HTN. Cited as an example of a "middle power" committing billions to sovereign compute, health-data standardisation and sustainability, while the UK "looks very alone." Read more
📎 NHS electronic patient records linked to serious-harm issues – Telecare Aware (BBC-sourced). Shared on the final Saturday to underline that "low risk" systems have caused harm at scale, tied to the point that 70.1 per cent of English trusts and ICBs hold no DCB0129/0160 clinical risk management. Read more
📎 OneLondon shared care record procurement – Find a Tender. An "interesting procurement" for the OneLondon shared care record, noted on Monday. Read more
📎 Newscord campaign on NHS and Palantir – Newscord. A member-shared campaign page behind the midweek thread on data sovereignty and the disputed question of personal data access. Read more
Industry and News Articles
📎 Global scramble for sovereign AI after the Anthropic shutdown – Fortune. The article that crystallised the midweek sovereignty debate and the sense that the UK is boxed out of others' plans. Read more
📎 Anthropic disables Fable and Mythos under export controls – Fortune, with companion coverage in Time and Anthropic's own statement. The source set behind the weekend reconstruction of the standoff. Read more Read more Read more
📎 Midjourney pivots to medical body-scanning – The Verge and The Register. The launch coverage behind the week's biggest curiosity, the second framing it as a "medical spa where patients bathe in golden light." Read more Read more Read more
📎 Anthropic may require identity verification for Claude use – Techzine. Read alongside speculation that "citizens of certain countries may get denied access," extending the week's access-and-sovereignty theme. Read more
📎 A court rules an AI company liable for false statements generated by its AI overviews – WIRED. Shared on Sunday as an early marker of where legal accountability for generative output may land. Read more
📎 France turns to AI data tools – The Guardian. Cited in the Palantir and data-sovereignty thread as a contrast with the UK's position. Read more
📎 Tech firms asked to shoulder more risk in NHS contracts – HSJ. Read with a characteristically dry caveat about the NHS "typically not realising savings because it doesn't like change." Read more
Technical Resources and Commentary
📎 Management as an AI superpower – One Useful Thing. Ethan Mollick's argument, echoed by members who have deployed agents across marketing, finance and ops, that management skill is a key determinant of agentic success. Read more
📎 Run GLM 5.2 locally: "the open model nobody can ban" – dev.to. The practical guide behind the local-models surge, paired with the Unsloth and Ollama routes to running it. Read more
📎 Agentic AI comes to medicine – Eric Topol (Ground Truths). Shared into the agents discussion as a clinical overview of where autonomous AI is heading. Read more
📎 Derm Zero: autonomous skin assessment from a smartphone – Skin Analytics. A Class III CE-marked autonomous capability from a standard smartphone, cited approvingly as an example of "doing it properly." Read more
📎 CAD-skill – GitHub (flowful-ai). A chat-driven CAD tool for the group's 3D-printing enthusiasts, generating accurate models from coordinate descriptions. Read more
📎 A neural network built out of goats in Age of Empires II – The Decoder. The week's technical curiosity, a Microsoft researcher's critique of "AI science" built inside a 1999 strategy game. Read more
📎 Welcome to the AGI era of AI governance – Interconnects. Read "with a healthcare and AI governance lens" as the export block reframed the governance conversation. Read more
🔭 Looking Ahead
HLTH Europe wrapped in Amsterdam this week, and attention turns to the autumn: a patient-safety organisation's digital lead who joined the group is chairing a debate at HETT in September on whether AI will make patients more involved and accountable for their own health, and is looking for a speaker against the motion. An AI Network meeting is scheduled for 1 July, and the monthly clinical safety officer "Coffee and Chat" community continues. The MHRA's consultation on proposed changes to medical device regulation is open and likely to draw the group's input, given the live classification debate. The export-block fallout will keep the sovereignty and open-source conversation running, with members watching whether the UK commits to a sovereign or middle-power model, whether Copilot ever reaches GP surgeries, and how the OneLondon shared care record procurement unfolds. Several members also flagged HSSIB's continuing investigation into electronic patient record safety as one to track.
🧬 Group Personality Snapshot
This is a community that can move from US export-control geopolitics to a 2-bit quantised local model to a brutally honest exchange about its members' own weight and health, all within an hour, and treat each with equal seriousness. It is sceptical of hype, dismantling a body-scanning "medical spa" in real time, yet unusually generous with lived experience, whether that is an out-of-hours audit from fifteen years ago, a deprescribing tool built single-handed, or a frank account of what a weight-loss drug did for someone after thirty years of trying everything else. Its centre of gravity is values rather than gadgets: a recurring insistence that whatever AI makes possible, the test is what it does for equity, for frontline workload, and for the "lonely, anxious individual" who came for help. It reads the regulator's consultations, argues about them line by line, and still finds time to build a neural network out of goats.
APPENDIX A: Detailed Activity Analytics 📊
📬 Total Messages: 577
📈 Peak Day: Friday 19 June (170 messages)
🔥 Most Active Period: Friday daytime (143 messages, morning and afternoon)
💬 Average / Active Day: 72 messages
🏖️ Weekend Activity: 25.5% (147/577)
💼 Weekday Activity: 74.5% (430/577)
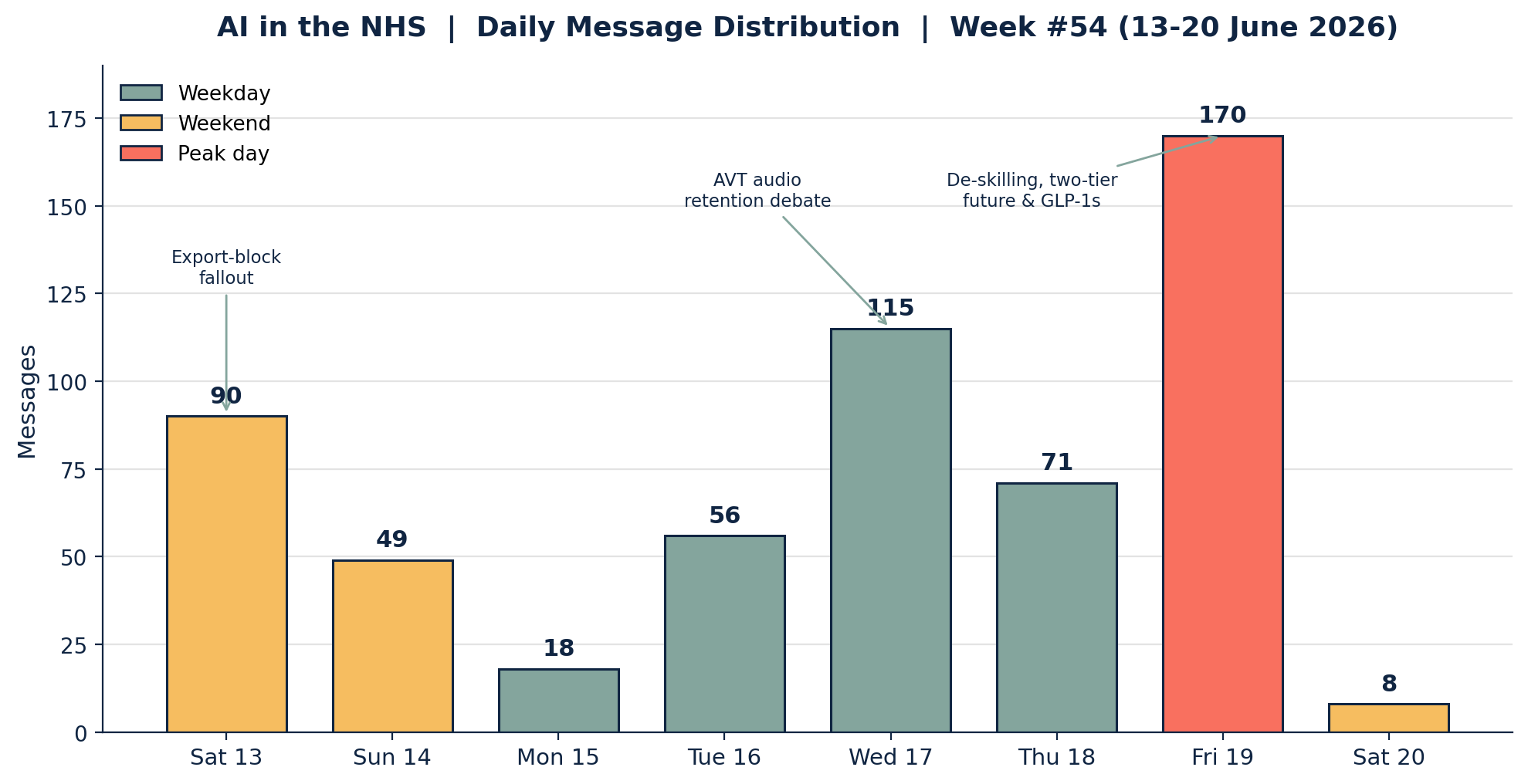
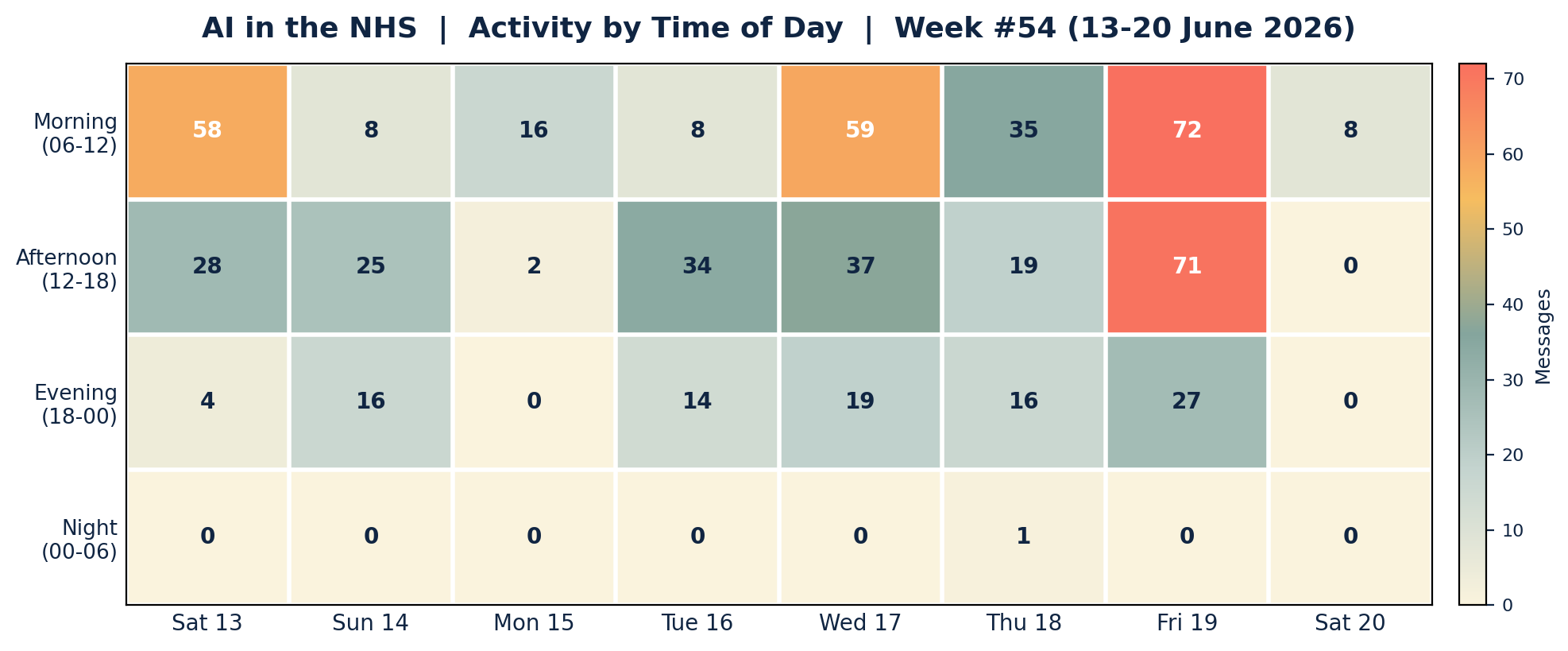
Peak engagement clustered in Saturday and Wednesday mornings (the export-block fallout and the AVT audio debate) and across the whole of Friday, which alone carried nearly a third of the week's traffic. The pattern was weekday-dominated but with livelier weekend bookends than last week, reflecting the news-driven sovereignty thread that refused to wait for Monday. Night-time activity was almost nil, with a single message in the small hours of Thursday.
APPENDIX B: Enhanced Statistics
Unique Contributors: 71 group members posted at least one message this week, out of the group's wider membership. The 15 most active below account for 401 of the 577 messages (69.5 per cent), with a long tail of occasional and one-off contributors making up the remaining 176 messages.
Top 15 Contributors (Role Descriptors Only):
1. Digital Health & Clinical AI Specialist (Group Moderator): 91 messages
2. Integrated care operations lead: 70 messages
3. GP running an in-house AI service in the mental-health space: 39 messages
4. Clinical safety and governance advocate: 27 messages
5. Practice-based GP and digital lead: 22 messages
6. Digital health GP exploring local models: 20 messages
7. Academic primary care researcher: 20 messages
8. Digital health technologist: 20 messages
9. Health-tech commentator: 19 messages
10. Clinician and health-tech founder: 17 messages
11. AI-forward GP: 16 messages
12. Frontline GP: 13 messages
13. Digital health strategist: 11 messages
14. Mental health consultant: 8 messages
15. NHS IT specialist (former utilities sector): 8 messages
Hottest Debate Topics:
1. 🔥🔥🔥 De-skilling, referral inflation and the two-tier future (Fri)
2. 🔥🔥🔥 Sovereignty and the open-source / local-model response after the export block (Sat-Wed)
3. 🔥🔥 AVT audio retention, accuracy and human error baselines (Wed)
4. 🔥🔥 GLP-1s, McPrescribers and Plan B for general practice (Fri)
5. 🔥🔥 Midjourney's medical pivot and the wellness-scan hype (Thu-Fri)
6. 🔥 Palantir, Newscord and NHS data sovereignty (Tue-Wed)
7. 🔥 GP2GP data degradation and the cost of lost coding (Sun)
8. 🔥 EPR safety, HSSIB and DCB0129/0160 gaps (Sat)
Discussion Quality Metrics:
• External resource sharing: more than 45 unique links across the period, spanning peer-reviewed papers, official consultations, trade press and open-source tooling
• Evidence base: heavy reliance on primary sources, with several Nature papers, an ICS trust report, a Commonwealth Fund ranking and an open MHRA consultation cited directly
• Constructive challenge: high, with the two-tier-future and audio-retention threads featuring sustained, respectful disagreement grounded in data and lived experience
• Breadth of participation: 71 unique contributors, with no single voice exceeding 16 per cent of total volume, a broad and well-distributed week
Cross-Expertise Engagement:
The week drew GPs and GP partners, mental-health clinicians, radiology and imaging voices, informaticians and NHS IT specialists, operations and management leads, health-tech founders, medical educators, pharmacists and medicines-information specialists, and patient-safety leaders. The most cross-disciplinary thread was Friday's de-skilling and two-tier debate, which pulled clinical, educational, economic, ethical and frontline perspectives into a single afternoon. A patient-safety organisation's chief digital officer and a medicines-information specialist were among those welcomed to the group during the week.
APPENDIX C: Daily Theme Summary
Saturday, 13 June 2026 (from 09:00)
Primary Theme: First reactions to the Fable and Mythos export block Key Discussion: The block was read as the start of regulatory capture and a decisive argument for owning your own inference and stocking up on open-source capacity, with early scepticism that UK "sovereignty" talk would ever become action. Secondary Discussions: A GPonline piece on the NHS workforce plan's "false assumptions"; a practice digital lead's saga with under-resourced NHS IT; whether AI can genuinely lift NHS productivity. Notable: The week opened where the last one ended, on sovereignty, and never really left it.
Sunday, 14 June 2026
Primary Theme: The standoff, reconstructed, and the sovereignty pivot Key Discussion: A balanced summary of the US-versus-Anthropic narratives prompted the moderator to reverse his earlier opposition to a UK sovereign frontier model, or failing that a middle-power collaboration. Secondary Discussions: A court ruling on AI-generated false statements; GP2GP data degradation (35 million coded items lost to text each year); an early research finding that external validation matters less to doctors than to other clinicians; HLTH Europe travel. Notable: A debate about a critical paper on a clinical-AI product showed how academia has become a commercial battleground.
Monday, 15 June 2026
Primary Theme: Quietest day; specialist models and RAG realism Key Discussion: A measured exchange on dedicated health models, the conclusion that most are "different flavours of the same ice cream," and that the real gap is medicolegal defensibility, not retrieval. Secondary Discussions: A OneLondon shared care record procurement; reminiscences of IBM Watson and Babylon; HLTH meet-ups. Notable: Just 18 messages, the calm before a very busy midweek.
Tuesday, 16 June 2026
Primary Theme: Chinese open models and personal data Key Discussion: Data showing Chinese systems as the five most popular models on a major routing platform fuelled the open-source case, alongside the disclosure that a popular coding tool was built on a Chinese model. Secondary Discussions: A 3.5GB personal health-data export and AI consent; Skin Analytics' Class III autonomous capability; France's turn to Palantir-style tooling; 3D printing. Notable: A patient asked their GP whether a named data firm could access their record, a sign the sovereignty debate has reached the consulting room.
Wednesday, 17 June 2026
Primary Theme: AVT accuracy, audio retention and storage economics Key Discussion: A supplier's "97 per cent accuracy" SLA opened a rigorous debate on human error baselines (around 7 per cent hallucination, 10 per cent omission in human notes), whether raw audio should be retained like radiology images, and the petabyte-scale cost of doing so. Secondary Discussions: UK isolation on sovereign AI; the Palantir and Newscord data campaign; a fresh MHRA consultation on device regulation; GLM 5.2 run locally. Notable: The day balanced patient acceptability against technical feasibility, landing on a 30-day retention compromise.
Thursday, 18 June 2026
Primary Theme: Midjourney's medical pivot and the acquisition question Key Discussion: Midjourney's claimed 60-second, MRI-resolution body scanner drew sharp scepticism and "medical spa" jokes, while a parallel thread offered hard-won advice on being acquired well rather than cashing out badly. Secondary Discussions: Patients bringing their own AVT to appointments; Copilot availability and tiers for GP surgeries; AI summarising as "brain rot"; an exhibitor reportedly asked to leave the HLTH floor. Notable: A patient's belief that an AI had diagnosed their ADHD set up Friday's biggest debate.
Friday, 19 June 2026
Primary Theme: De-skilling, the two-tier future and Plan B for general practice Key Discussion: The week's busiest day ran a single long argument from AI-driven referral inflation through clinical de-skilling to a subscription-GP future, then into GLP-1 economics, McPrescribers and the case for letting NHS GPs charge for evidence-based care. Secondary Discussions: Candid personal GLP-1 testimony; management skill as the key to agentic AI; 3D-printed medicines; the Commonwealth Fund defence of the NHS model. Notable: 170 messages, the most of any day, and among the most personal exchanges the group has had.
Saturday, 20 June 2026 (to 09:00)
Primary Theme: Electronic patient record safety Key Discussion: A reminder that "low risk" EPR systems have caused serious harm at scale, tied to the finding that 70.1 per cent of English trusts and ICBs hold no DCB0129/0160 clinical risk management, the legally mandated minimum. Secondary Discussions: HSSIB's continuing EPR investigation; the limits of treating EPRs as non-devices as AI features arrive. Notable: Coverage cut off at 09:00; the EPR safety thread continued into the next reporting period.
AI in the NHS Weekly Newsletter is produced by Curistica Ltd for members of the AI in the NHS WhatsApp community. All contributors are anonymised. Views expressed are those of individual community members and do not represent any organisation.