
Executive Summary
A week that began and ended with the same underlying question: who do we trust to write the record, and who carries the can when it is wrong. It opened on Saturday with a four-hour debate on AI scribes, sparked by a cautionary review of transcription error rates, that drew out one of the most candid exchanges in the group's history on documentation, defensibility and neurodivergence. It closed on Friday with a sprawling argument about platforms and sovereignty, the NHS App "guillotine" for smaller suppliers, and the long shadow of the National Programme for IT.
Between those bookends the group worked through the new Pope's encyclical on artificial intelligence, a Health Service Journal investigation into how few AI incidents ever reach the regulator, a High Court judgment that fixed legal liability on professionals who lean on unreliable AI, and the leaked plan to push the Federated Data Platform into primary care. There was a Pope quoted in the register of a Chicago mob boss, an Amiga 500 memory upgrade remembered more fondly than Claude Opus 4.8, and a robot cleaner welcomed as our new overlord. Four hundred and thirty-eight messages in seven days; here are the threads that shaped them.
Activity at a Glance
Week 51 generated 438 messages across the seven-day coverage period, with peak activity on Saturday 23 May (111 messages) driven almost entirely by an evening-long AI scribe debate, and a strong second peak on Friday 29 May (83 messages). Weekday activity dominated at 63.9% of total volume, though the single busiest day was a Saturday. Monday 25 May was the quietest at just 15 messages, a bank holiday lull before the week found its stride.
📌 Major Topic Sections
1. The AI Scribe Illusion and the Great Documentation Debate
The week's defining thread opened on Saturday afternoon when a GP shared a cautionary article on ambient voice technology, summarising a recent review of error rates and their nature, and suggested it was worth considering by users and the AVT-curious alike. The reaction was immediate and slightly rueful. "No wonder AI is banned in my surgery," came one reply, while a GP and digital health academic observed that "it feels like the AVT honeymoon (in the UK) might be nearing an end."
What followed ran until well past eleven that night and reached for first principles. The article had praised the economy of the shortest notes, prompting the group's moderator to push back: "I struggle to think of a time that economy of notekeeping was ever helpful when investigating a complaint." An innovation-focused GP argued that "short succinct clinical notes written in technical language are much easier to defend," citing the maxim that "the more words lawyers have access to, the more likely they will come out on the winning side." A documentation-focused GP took the opposite tack, pointing out that his own lawyer has access to the same words and that "the fewer words they have to defend me the less well they can represent me."
The thread's most affecting turn came when a GP and committed AVT user explained candidly why his notes run long, attributing it to autism, ADHD and a lack of self-confidence, and noting that ambient scribing reduced his cognitive load disproportionately. "Sorry, you probably didn't want to know all that," he added, "but behind every bit of tech is a person." It was a reminder that adoption curves are made of individuals, not averages.
Running underneath was a quieter disagreement about what notes are for. For one GP at a large practice, "my notes are a message to future me about the patient," and AVT output, however accurate, missed the salient points and took too long to re-read. An innovation-focused GP set out a seven-point case for why he remains, in his own phrase, "Anti-AVT in the AI group," chief among them that note-typing is his thinking and clinical reasoning time. A consultant cardiologist took the discussion in the other direction entirely, sketching a vision of a mature system that verifies the summary care record, pre-computes risk scores, drafts the prescriptions and books the follow-ups before the patient even enters the room. A documentation-focused GP's dry rejoinder captured the room: "This product would be an absolute gift for medical negligence solicitors." For all the disagreement, one point drew consensus, voiced by the moderator: forcing people to use AVT if it does not work for them is a bad idea.
📣 Call for Participants: AI Scribes in Primary Care
A group member is running a University of Manchester qualitative study on GP perspectives on AI scribes, and shared the formal invitation with the group on Tuesday. The study, Perspectives on the use of AI scribes in Primary Care, explores the perceived advantages, disadvantages, barriers and facilitators to their implementation, and the group's documentation debate this week is exactly the kind of insight it is after.
Who can take part: GPs in the UK and Ireland of all experience levels, including both users and non-users of AI scribes.
What is involved: a one-to-one semi-structured interview of 30 to 45 minutes, held remotely by secure video or telephone at a time that suits you. Participation is voluntary and you may withdraw at any time. A £15 coffee voucher is offered on completion.
To take part or find out more: contact the Principal Investigator, Dr Ronan Sharkey (GP), at info@edgeworthstownmedical.com or +353 43 6671157. Academic Supervisor: Dr Benjamin Brown, Clinical Senior Lecturer, Centre for Primary Care and Health Services Research, University of Manchester.
2. Private, NHS, and the Quiet Death of the Grand Round

Monday was the quietest day of the week but produced one of its more reflective threads, after an innovation-focused GP shared an article suggesting private radiology reports are rated low quality by NHS radiologists, asking why we persist with the binary view that "private = inadequate and NHS = outstanding." A hospital radiologist found the subtext "an irritating trope," noting wearily that it is often "the same people" reporting in both settings.
The conversation widened into something more elegiac: the erosion of relationships across the primary and secondary care interface. A GP recounted a recent interface meeting where colleagues concluded that quality suffers when accountability is anonymised, because "anonymity between clinicians allows for quality reduction without the personal ramifications." A hospital radiologist traced the decline to the moment "Grand Rounds died a decade ago," after which "everyone works in silos." A hospital consultant remembered drinks and direct calls with primary care colleagues twelve years ago and proposed a remedy with some warmth: "Let's bring that back in our patch. I'll bring the drinks, you bring your bbq skills." Running alongside, an article on trusts outsourcing advice and guidance to save money was shared as "a significant breach of the relationship with their local GPs," and a separate study on AI rating identical CVs differently by gender drew a tired observation that "every opportunity we seem to go back to misogyny and discrimination."
3. A Pope, a Constitution, and a Moral Frame for AI
Tuesday morning the group turned to the new Pope's first encyclical on artificial intelligence, shared via a widely-admired summary. The moderator, declaring himself "an atheist heading towards agnostic," welcomed thoughtful input from religious leaders, and paired the encyclical with Anthropic's recent constitutional work as evidence that "some people are facing the challenges ahead in a human way." His paraphrase of an old student-dorm poster set the tone: "I like this Pope, this Pope talks hope."
The thread balanced genuine seriousness with some of the week's sharpest comedy. On the substance, a practice operations and data lead made the case that "we're largely leaving the development of the current major tech innovation to the sort of folk who believe that all the world's money should belong to them," and was glad of a moral voice entering the fray. On the comedy, the same contributor reimagined the Chicago-born pontiff in the register of a mob boss ("that's a nice government you have there, be a shame if anything happened to it"), while the moderator offered a Vatican enforcement policy for data breaches: "You send one of them to the ICO, we send one of them to Purgatory. That's the Vatican way." A documentation-focused GP added useful context on the Christian Medical Fellowship and pointed to first-principles writing on medical AI, and a secondary care specialist flagged the theological and ethical work coming out of Bath's ART-AI doctoral centre.
4. The Regulator's Blind Spot: Yellow Cards and the Incidents That Never Get Reported
Wednesday afternoon brought a Health Service Journal report that the regulator is missing many AI incidents, with only a handful of yellow card reports logged. A GP and committed AVT user noted, drily, that "two or three of those were mine," before the thread became a forensic examination of why so little is reaching the MHRA. The barriers were laid out plainly: the reporting routes are "prohibitively difficult," and clinicians are told that transcription errors, filing errors and omissions do not count, even though manufacturers themselves "admit perhaps 2% hallucination events, so there should be hundreds of reports."
A clinical safety lead at an AVT manufacturer offered the supplier-side view, explaining the obligation to report clinical safety events and that not all hallucinations rise to that bar, a point the group accepted but found cold comfort given the volume. A clinical safety specialist argued the deeper fix is structural: reporting should be "a standalone, separate system that clinicians are separately trained on," rather than a different three-click journey buried in every product's help menu. A digital health clinician called for strong requirements on post-market surveillance plans for key technology categories, followed by formal auditing of those plans, against an MHRA "direction of travel" widely read as deregulation. The moderator noted that his own organisation's reporting tool retains no data and simply helps a clinician assemble a report to email to the regulator, and that anyone who has sat through one of their hazard workshops will "get flashbacks about training." An innovation-focused GP delivered the verdict the thread had been building towards: government, NHS England and ICBs "went ahead with large scale procurement of AVTs without a proper reporting mechanism."
5. When the Machine Errs: the Bailii Judgment and the Doctor's Burden
Thursday afternoon a practice operations and data lead shared a High Court judgment that he flagged as quietly consequential for medicine. Its paragraph 96 confirmed, in the context of a lawyer's catastrophic misuse of AI, that "legal professionals bear ultimate responsibility for their work and cannot outsource the process of legal research or of legal reasoning to an AI," and that AI "has the potential to be wholly unreliable." The inference for clinicians was not hard to draw: "It's not a huge leap for even a pretty poor medical negligence lawyer to expect courts to transfer that liability to doctors by the same principle," with the prospect of indemnifiers writing AI use into policies as exclusions or price rises.
The asymmetry rankled. A digital health consultant put it most memorably: "$2,000/hour lawyers missed three pages of AI hallucinations in a court filing. Doctors using an AI scribe are somehow expected not to miss one." Others drew out the structural difference between the professions. A practice operations and data lead noted that a law firm "will generally back their lawyers because they don't want corporate liability," whereas the NHS "has a track record of 'nope, that was all the doctor's fault.'" The moderator offered a characteristically even counterweight, suggesting that a well-built system "would outperform baseline performance of human equivalent," and that the meaningful comparison is not against perfection but against the status quo. The day's other headline, the release of Claude Opus 4.8, landed into this context with the moderator's one-line gloss: "It's come for the lawyers."
6. Platforms, Sovereignty, and the Ghost of NPFIT
The week's longest-running theme threaded through Thursday and Friday and concerned, at root, who controls the platform and the data. It began with a leaked plan to push the Federated Data Platform into primary care. The reception was scathing. An innovation-focused GP judged his "inhouse built PHM far richer than FDP is ever likely to be"; a clinical AI founder, who works in the space "24/7," remained "perplexed what it is actually solving for"; and a practice operations and data lead delivered the line of the thread, finding himself reluctantly praising EMIS Enterprise because "it makes FDP look like a pivot table created by someone who hasn't used Excel before." The consensus was that FDP's only genuine advantage is country-wide scale, and that scale mostly serves to "give reports to people who can then tick boxes that they've had a report."
By Friday the argument had widened to a Health Service Journal piece on the NHS App "guillotine" facing smaller online-consultation suppliers as the centre brings the function in-house. A GP and early Medicus adopter warned against any attempt to "nationalise health IT," and a hospital radiologist invoked the inevitable ghost: "The spectre of NPFIT haunts us to this day." A secondary care interoperability specialist, by his own account a quarter-century advocate of best-of-breed connectivity, gave the week's most considered single post, arguing that the monolithic EPR is a fantasy, that two-to-five million population looks like the right size to do digital health well, and that "there is a right tier for everything," with the regional layer the neglected and most promising one. The thread also surfaced a transatlantic dispute on enforcement, with one GP urging a UK equivalent of the 21st Century Cures Act and its million-dollar information-blocking fines, and a hospital radiologist puncturing the optimism: "We have codified fines too. You reckon anyone enforces them?" A clinical AI scientist confirmed the point, noting "over a thousand complaints under 21CCA but no one has been fined." A health-tech developer's verdict on the interoperability standard at the centre of it all was the most quotable: "FHIR is a string vest, it has more holes than fabric."
Underneath the platform argument ran a parallel one about compute. An innovation-focused GP made the case for running open-source models on owned hardware, predicting many organisations will settle on a "70/30 split" of internal open models and proprietary ones, while a clinical safety specialist countered that hardware scarcity, rising power costs and the pull of cloud architecture make on-premise a low-single-digit pursuit. An NHS AI infrastructure builder urged everyone to "stress test their RoI assumptions" given what is happening to the cost of token subsidy, and noted that the on-premise versus cloud question is "a bit like PlayStation versus Xbox, mostly tribal, but it does define what you can and can't do at what cost point."
😄 Lighter Moments
The release of Claude Opus 4.8 prompted less awe than expected. A GP and AI tool creator read the alignment team's praise of the model's prosocial traits and concluded that nothing had ever matched the thrill of upgrading his Amiga 500 from 256kb to 512kb of RAM as a twelve-year-old: "I could finally play Superfrog! Every new tech upgrade since has not even come close." A separate contributor noted that 4.7 had shipped only the week before, sighing that "marketing has really changed in 2026."
Friday's news that a robot cleaner had been deployed somewhere triggered the predictable welcome to "our new robot cleaner overlords," followed by a practice operations and data lead leaning fully into the dystopia: "Messy things are humans, messy, best to clean them away." A colleague supplied the obligatory Dalek "exterminate."
The week's other reliable comic seam was hardware envy. A costing exercise for a "medium-high spec" machine returned £4,500, prompting the observation that "you have to pledge to donate a kidney to get an increase in memory," and a fond tangent on ageing graphics cards, an eight-year-old 1070ti, a 750Ti upgraded to a 1650 GTX, and the urgent need to fly a "Trusty Cobra Mk3 at higher frame rates this summer." Elsewhere, the close of the fantasy football season produced the verdict that "Claude would have done a better job" managing the squad, and a hospital radiologist, reviewing the Commonwealth Fund's flattering ranking of the UK, channelled a satirical America with "all the standards, so many standards, every time you want."
💬 Quote Wall
"Behind every bit of tech is a person." – GP and committed AVT user
"My notes are a message to future me about the patient." – GP at a large practice
"$2,000/hour lawyers missed three pages of AI hallucinations in a court filing. Doctors using an AI scribe are somehow expected not to miss one." – Digital health consultant
"I like this Pope, this Pope talks hope." – Group moderator
"You send one of them to the ICO, we send one of them to Purgatory. That's the Vatican way." – Group moderator
"It makes FDP look like a pivot table created by someone who hasn't used Excel before." – Practice operations and data lead
"The spectre of NPFIT haunts us to this day." – Hospital radiologist
"FHIR is a string vest, it has more holes than fabric." – Health-tech developer
"We have codified fines too. You reckon anyone enforces them?" – Hospital radiologist
"You have to pledge to donate a kidney to get an increase in memory." – Practice operations and data lead
📎 Journal Watch
Academic Papers & Key Studies
📎 The AI Scribe Illusion: Why More Technology Is Not Always Better – Trust the Evidence (Substack) A cautionary piece on ambient voice technology in general practice, summarising a review of error rates and their nature. It opened the week's defining documentation debate and the suggestion that the UK AVT honeymoon may be ending. Read more
📎 Adler-Milstein on AI in Clinical Documentation – JAMA Shared on Sunday morning as a "neat articulation of that race," prompting the moderator to begin drafting a UK-perspective response. Read more
📎 Mirror, Mirror 2024: International Health System Comparison – The Commonwealth Fund Surfaced after a US healthcare CEO presented a slide showing the UK ranking surprisingly well. The group debated the methodology and what "administrative efficiency" actually measures. Read more
📎 Doctronic AI Prescribing Pilot: Outcomes, May 2026 – Utah Department of Commerce Early results from a US AI prescribing pilot, shared with the caveat that data of this kind needs validation, clear ownership and explicit liability before it could inform UK practice. Read more
📎 First Principles for Medical AI – Christian Medical Fellowship Shared in the encyclical thread as a broad representation of underpinning principles for a Christian view on medical AI, with the noted caveat of its July 2023 date. Read more
Industry & News Articles
📎 Regulator Missing Many AI Incidents – Health Service Journal The trigger for Wednesday's reporting deep dive, revealing how few AI incidents reach the MHRA via the yellow card route, and the structural barriers that keep them under-reported. Read more
📎 Revealed: NHSE Project to Put FDP into Primary Care – Health Service Journal The leaked plan to extend the Federated Data Platform into general practice, which opened the week's platforms-and-sovereignty thread and a wave of scepticism about what FDP solves for. Read more
📎 Smaller Tech Firms Face NHS App 'Guillotine' – Health Service Journal The report that the NHS App is bringing online consultation in-house, raising the prospect of smaller suppliers being cut out and reviving NPFIT-era anxieties about nationalising health IT. Read more
📎 $500m In-House AI at the World's Largest Law Firm – Financial Times Shared as evidence that for sovereign and ultra-sensitive data, owning your own system on your own hardware is becoming a responsible choice, with a wish that the NHS had the willpower to follow. Read more
📎 $2,000/hour Lawyers Missed Three Pages of AI Hallucinations – LinkedIn The commentary that crystallised the liability thread's central asymmetry between how AI error is treated for highly paid lawyers and for clinicians using a scribe. Read more
📎 GPs Fear Delays as Hospitals Outsource Advice and Guidance – GPonline Shared in Monday's interface thread as an example of trusts outsourcing A&G to save money, read by some as a breach of the local relationship between hospitals and GPs. Read more
📎 Interview with Shiv Rao, CEO of Abridge – HLTH Recommended for anyone interested in ambient voice technology, offering a vendor's-eye view of where the category is heading. Read more
📎 Identical Resume, Different AI Response by Gender – Fortune Evidence of gendered bias in AI responses to otherwise identical CVs, shared as a reminder of how readily these systems reproduce human discrimination. Read more
📎 Google Ruins Fitbit – Joe Baldwin (blog, contains strong language) A first-hand account of the Fitbit-to-Google-Health transition stripping features and silently widening data permissions, anchoring the group's unease about big tech and health IP. Read more
📎 Google to Infuse Ads into AI Answers – The Register On Google folding advertising into AI search results, with a warning that forced adverts and whitelisting risk contaminating the underlying model. Read more
📎 Amazon Joins the AI 'Tokenmaxxing' Leaderboard – Business Insider After Microsoft and Uber, Amazon is now measured on AI token usage, feeding the week's running thread on the economics of token consumption. Read more
📎 BBC Question Time's AI Panel – Radio Times The much-derided AI panel featuring Gandhi and Che Guevara, judged by the group to be overwhelmingly and uncritically pro-AI, with a single token sceptic. Read more
Technical Resources & Guidelines
📎 An Encyclical on AI – Simon Willison The summary of the Pope's encyclical that anchored Tuesday's discussion, praised as a thoughtful entry point complete with Lord of the Rings references. Read more
📎 Claude Opus 4.8 – Anthropic The latest frontier release, with the group noting strong safety-card performance in mental health and disordered eating, and improved honesty about the limits of its own knowledge. Read more
📎 Mythos Detects 23,000 Vulnerabilities Across 1,000 OSS Projects – Slashdot Shared as a striking demonstration of AI applied to security research at scale across open-source software. Read more
📎 coplug.ai and arjus data chat – Population health query tools Two natural-language-to-data tools surfaced on Friday, one a commercial product for interrogating population health data, the other an ICB analytics team's semantic-layer experiment turning plain English into SQL over the London Data Service. Read more
📎 ART-AI Seminar, University of Bath – UKRI Centre for Doctoral Training in Accountable, Responsible and Transparent AI Shared in the encyclical thread as a pointer to serious theological and ethical work on AI, including contributions from the Church of England's Director of Faith and Public Life. Read more
Policy Documents & Official Reports
📎 Is the NHS Ready for the AI-Powered Patient? – The King's Fund A newly published long read shared by its author, prompting a thoughtful exchange on why "the NHS" and "AI" are both terms that obscure more than they reveal, and the grown-up system conversation still to be had. Read more
📎 Use of Evidence Generated by Software in Criminal Proceedings: Call for Evidence – UK Government Shared during the documentation debate as the live question of how much we should trust software-generated records, with direct relevance to the legal status of AVT output. Read more
📎 High Court Judgment: EWHC 2026/1199 (Ch), Paragraph 96 – BAILII The judgment that fixed ultimate responsibility on legal professionals who outsource research or reasoning to unreliable AI, read by the group as a precedent likely to be transferred to clinicians. Read more
🔭 Looking Ahead
The group's moderator has floated an AI in the NHS panel-style podcast drawing on members to discuss the topics covered here, possibly with a journal-club element for appraisal purposes, and the early response has been warm. He is also preparing a keynote for late June and has put out an open call for examples of patients using AI to build their own solutions, beyond simple question-answering, where a genuine build or creative use has positively helped. The RAND Europe DECIDE Impact Forum on tech-enabled health and social care takes place in person in London on Wednesday 4 June, with organisers particularly keen to see primary care colleagues. The MHRA's posture on device regulation remains under scrutiny, with the group still pressing for a proper, standalone incident-reporting mechanism. And there is reading to digest: the latest NEJM AI collection was flagged as "an ambient scribe treasure trove," and a UK-perspective response to the week's JAMA piece is in preparation.
🧬 Group Personality Snapshot
This week showed the group at its most range-y. The same forum that sustained a four-hour Saturday-night debate on the philosophy of clinical documentation, drawing out a genuinely moving account of how neurodivergence shapes one doctor's note-keeping, could pivot within hours to a Pope reimagined as a Chicago mob boss and a robot cleaner welcomed as our overlord. The week's defining intellectual posture was constructive disagreement done well: a documentation-focused GP patiently Socratic-questioning an innovation-focused GP across dozens of messages without either losing goodwill, and a builders-versus-sceptics tension that ran through every technical thread without curdling.
What holds it together is a shared seriousness about consequences. Whether the topic was who carries the liability when AI errs, whether smaller suppliers survive the NHS App, or why so few real incidents reach the regulator, the group kept returning to the people on the end of the technology: the patient whose data is dumped over a silo wall, the doctor left holding the can, the neurodivergent clinician for whom the right tool is genuinely liberating. The Amiga 500 nostalgia and the GPU price laments are not a distraction from that seriousness; they are its release valve. Few professional communities argue this hard and still want to share a barbecue.
APPENDIX A: Detailed Activity Analytics 📊
📬 Total Messages: 438 across 7 days
📈 Peak Day: Saturday 23 May (111 messages)
🔥 Most Active Period: Saturday evening (AVT debate) and weekday mornings/afternoons
💬 Average/Day: 62.6 messages
🏖️ Weekend Activity: 36.1% (158/438)
💼 Weekday Activity: 63.9% (280/438)
🧠 Quietest Day: Monday 25 May (15 messages)
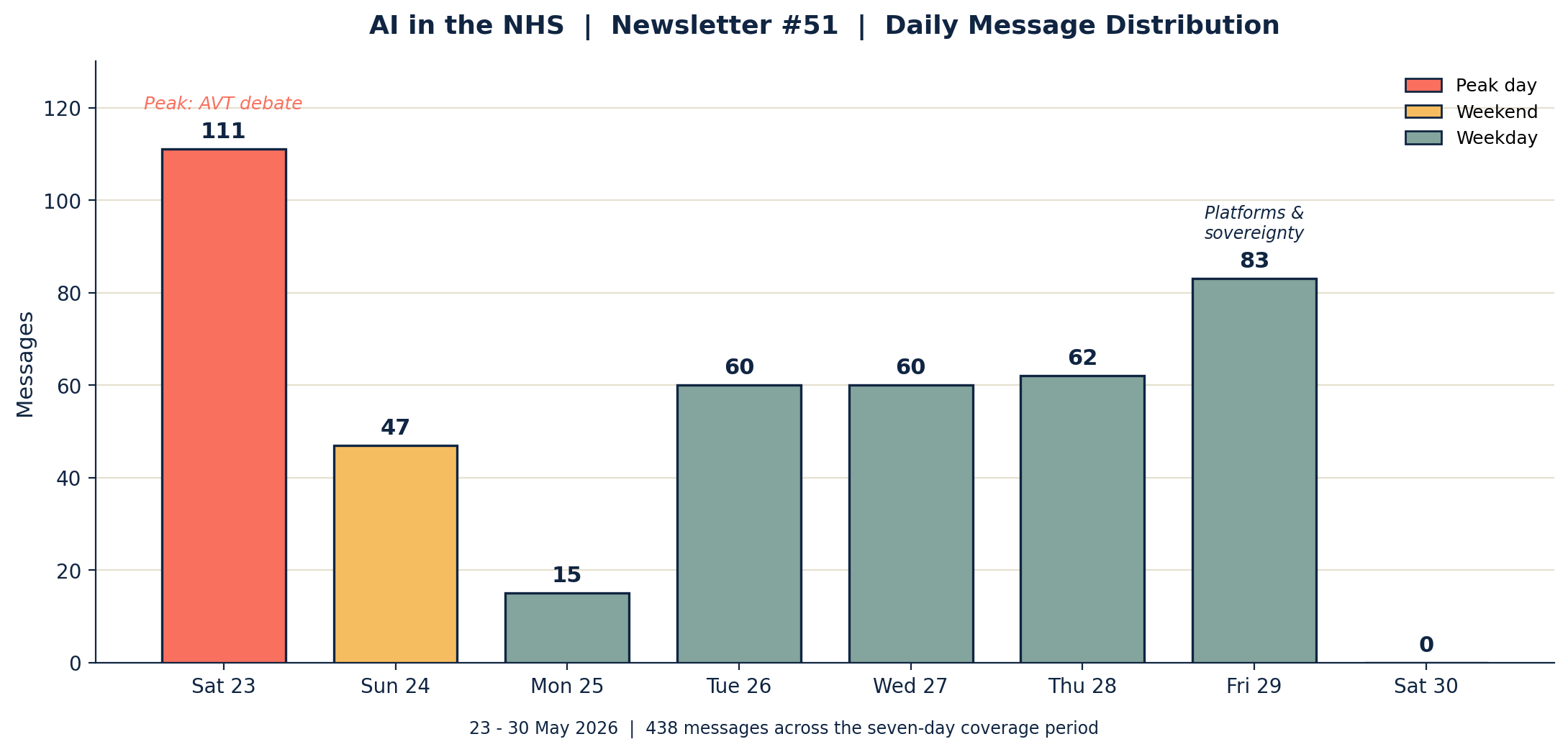
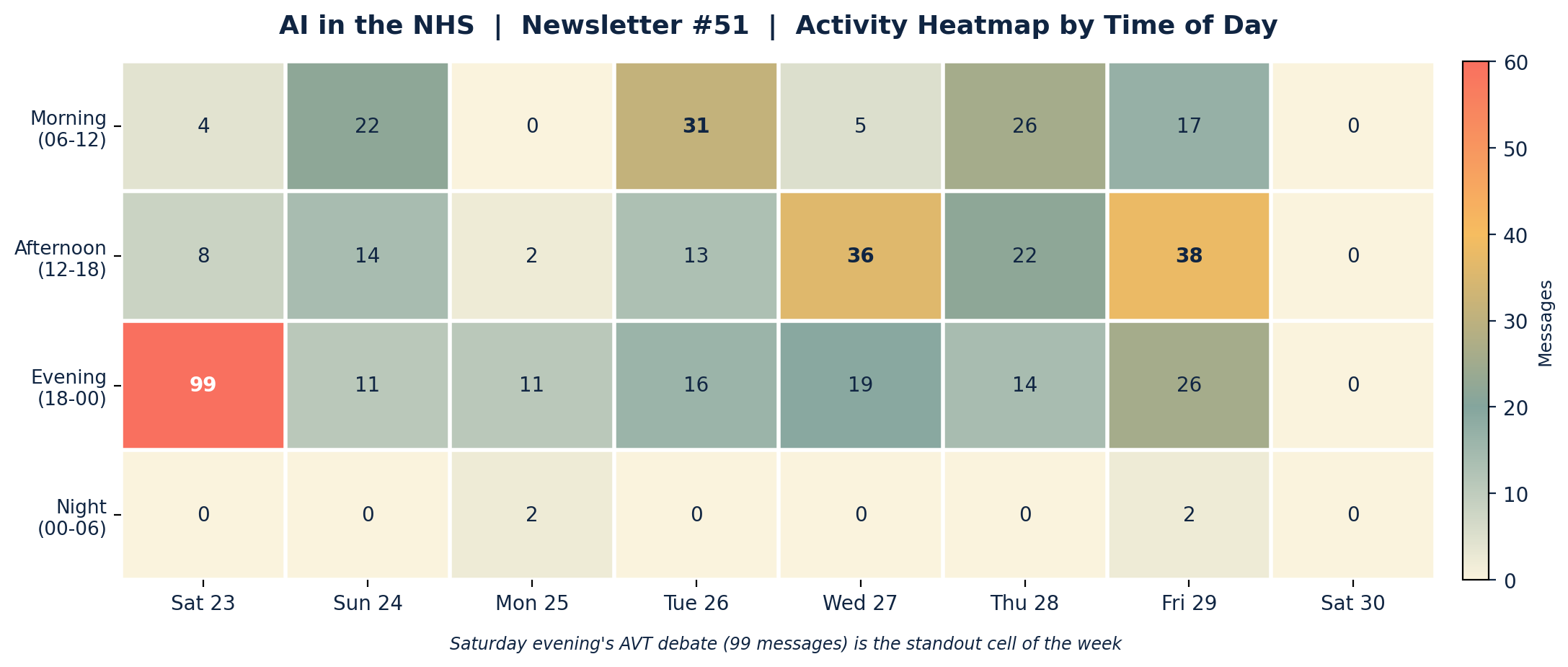
Insights: Saturday's peak was a single sustained evening thread rather than a day of broad activity, with 99 of its 111 messages falling after 18:00 as the AVT documentation debate ran past 23:00. The working week showed a different shape, clustering in mornings and afternoons as articles were shared and dissected before the school run and after lunch. Friday's strong second peak was unusually well distributed across afternoon and evening, carried by the platforms-and-sovereignty marathon. Monday's bank-holiday lull (15 messages) was the quietest day in several issues.
APPENDIX B: Enhanced Statistics
Top 10 Contributors (Role Descriptors Only)
1. Group Moderator (Digital Health & Clinical AI Specialist): 52 messages
2. Practice Operations & Data Lead: 48 messages
3. Innovation-Focused GP: 37 messages
4. Documentation-Focused GP: 34 messages
5. GP and Committed AVT User: 33 messages
6. Hospital Radiologist: 27 messages
7. Consultant Cardiologist: 20 messages
8. Health-Tech Developer: 18 messages
9. GP and Digital Health Academic: 16 messages
10. GP and Early Medicus Adopter: 12 messages (tied with a Secondary Care Interoperability Specialist)
Hottest Debate Topics
1. 🔥🔥🔥 AI scribe documentation debate: error rates, defensibility, neurodivergence, the ideal system (Sat evening, ~90 messages across Sat-Sun)
2. 🔥🔥🔥 Platforms and sovereignty: FDP into primary care, NHS App guillotine, NPFIT, interoperability (Thu-Fri, ~70 messages)
3. 🔥🔥 Yellow cards, MORE reporting, and the regulator's blind spot (Wed afternoon, ~32 messages)
4. 🔥🔥 AI liability and the Bailii judgment, indemnity and the doctor's burden (Thu, ~24 messages)
5. 🔥🔥 The Pope's encyclical, religion, and a moral frame for AI (Tue morning, ~22 messages)
6. 🔥 On-premise versus cloud inference and the token economy (Fri, ~20 messages)
7. 🔥 Private vs NHS quality and the death of the Grand Round (Mon, ~14 messages)
8. 🔥 PC builds, GPU prices, and retro gaming (Fri evening, ~16 messages)
Discussion Quality Metrics
• Evidence-Based vs Opinion Ratio: 38 unique external links shared across the period; roughly a third of substantive threads were anchored to a paper, article, judgment or official document
• Average Thread Depth: high, with the Saturday AVT thread and the Friday interoperability thread each sustaining 40-plus message exchanges
• Constructive Challenge Rate: notably high, the week characterised by sustained, good-natured disagreement rather than consensus
• External Resource Sharing: 38 unique links spanning journals, HSJ investigations, a High Court judgment, policy reports and technical tools
Cross-Expertise Engagement
• At least 14 distinct professional backgrounds contributing: GPs, a consultant cardiologist, a hospital radiologist, secondary care interoperability specialists, clinical safety leads (manufacturer and independent), data and population-health specialists, AI founders and engineers, health-tech developers, think-tank researchers and a clinical AI scientist
• Most cross-disciplinary thread: the platforms-and-sovereignty marathon, spanning GP, secondary care, manufacturer, ICB analytics and infrastructure perspectives
• Notable knowledge transfer: a secondary care interoperability specialist explaining regional care records and IHE standards to a primarily primary-care audience
• The majority of major threads involved three or more distinct professional perspectives
APPENDIX C: Daily Theme Summary
Saturday 23 May 2026
Primary Theme: AI scribes and the philosophy of clinical documentation Key Discussion: A cautionary article on AVT error rates opened a four-hour evening debate on note-keeping, defensibility, thinking time and a candid account of how neurodivergence shapes documentation. A consultant cardiologist sketched the ideal future system; a documentation-focused GP warned it would delight negligence solicitors. Secondary Discussions: A proposal for an AI in the NHS panel podcast; the publication of newsletter #50; the common-law status of software-generated evidence. Notable: Peak day at 111 messages, 99 of them after 18:00, the most concentrated single-thread evening in recent issues.
Sunday 24 May 2026
Primary Theme: AVT continued, continuity of care, and quality assurance Key Discussion: The documentation thread matured into a discussion of continuity, deep patient knowledge and the absence of visible QA processes in AVT products, including a seven-point case for scepticism and a counter-argument about edit-rate tracking. Secondary Discussions: Claude in PowerPoint outclassing Microsoft Copilot; the one-year anniversary of a Medicus deployment; Google folding ads into AI search; the close of the fantasy football season. Notable: 47 messages; a reflective Sunday that kept the week's central thread alive.
Monday 25 May 2026
Primary Theme: Private versus NHS quality and the primary-secondary care interface Key Discussion: An article on private radiology report quality prompted a discussion of accountability, anonymity between clinicians, and the erosion of interpersonal connection since "Grand Rounds died a decade ago," with a consultant proposing to rebuild it over a barbecue. Secondary Discussions: Trusts outsourcing advice and guidance; AI reproducing gender bias in CV screening. Notable: Quietest day at 15 messages, a bank-holiday lull.
Tuesday 26 May 2026
Primary Theme: The Pope's encyclical and a moral frame for AI Key Discussion: A widely-admired summary of the encyclical anchored a thread balancing genuine reflection on who is building AI and to what end with some of the week's sharpest comedy. Christian Medical Fellowship resources and Bath's ART-AI work were shared. Secondary Discussions: The Commonwealth Fund ranking and administrative-efficiency debate; Google Health "ruining" Fitbit; social care data dumped into the GP record as "an inelegant solution to a wicked problem"; a RAND Europe forum invitation. Notable: 60 messages, front-loaded into a busy morning.
Wednesday 27 May 2026
Primary Theme: The regulator's blind spot on AI incidents Key Discussion: An HSJ report on missing AI incidents opened a forensic thread on why so little reaches the MHRA, what counts as reportable, the difficulty of yellow card and MORE submissions, and calls for a standalone reporting system and audited post-market surveillance plans. Secondary Discussions: The King's Fund "AI-powered patient" long read; the Abridge CEO interview; alignment with Europe versus the USA versus the international forum. Notable: 60 messages, concentrated in a busy afternoon.
Thursday 28 May 2026
Primary Theme: AI liability, the Bailii judgment, and the FDP leak Key Discussion: A High Court judgment fixing responsibility on professionals who lean on unreliable AI was read as a precedent likely to transfer to clinicians, alongside the leaked plan to push FDP into primary care and widespread scepticism about what it solves for. Secondary Discussions: Patient-built AI solutions and whether the NHS could consume the data; the release of Claude Opus 4.8 and its safety card; the BBC Question Time AI panel. Notable: 62 messages spanning legal, platform and frontier-model news.
Friday 29 May 2026
Primary Theme: Platforms, sovereignty, interoperability and the NHS App guillotine Key Discussion: The NHS App bringing online consultation in-house revived NPFIT anxieties and a substantial thread on centralisation versus regional care records, the limits of FHIR, and the 21st Century Cures Act enforcement debate, paired with an argument on on-premise versus cloud inference and the token economy. Secondary Discussions: Population-health query tools; robot cleaners; GPU prices and retro gaming; the NEJM AI ambient scribe collection. Notable: Strong second peak at 83 messages, well distributed across afternoon and evening.
Saturday 30 May 2026 (cutoff 09:00)
Primary Theme: Coverage window closed Key Discussion: No messages fell within the coverage window before the 09:00 cutoff; Friday night's hardware thread was the last substantive exchange of the period. Notable: 0 messages within the window.
AI in the NHS Weekly Newsletter is produced by Curistica Ltd for members of the AI in the NHS WhatsApp community. All quotes are attributed to professional role descriptors only; the only named individuals are the researchers in the Call for Participants notice, included at their request. Views expressed are those of individual community members and do not represent any organisation.



