
Executive Summary
A landmark week for the group, opening with a constitutional flashpoint as the new NHS Bill's data sharing clauses landed and closing with the first standalone AI scribe in Europe receiving Class IIa MDR certification. Between those bookends, the group lost a giant of medical scholarship in Richard Lehman, dissected a leaked NHS workforce plan that swaps human staff for AI, mounted a forensic critique of the MHRA's draft device regulations, and ran one of the most philosophically ambitious threads in recent memory on whether AI in medicine is approaching a Semmelweiss moment or a long descent into mud-hut-and-frogs territory.
Throughout the week, the discussion oscillated between the technical and the existential, the constitutional and the comedic. Half a thousand messages in seven days; here are the threads that shaped them.
Activity at a Glance
Week 50 generated 514 messages across the seven-day coverage period, with peak activity on Wednesday 20 May (133 messages) driven by the workforce plan leak and the late-night ethics marathon. Saturday 16 May was unusually busy at 98 messages as the Bayes Business School after-party rolled into the weekend. Weekday activity dominated at 73.7% of total volume, with Friday 22 May the quietest at just 21 messages as members caught their breath.
📌 Major Topic Sections
1. The NHS Bill, Section 260, and the Quiet Death of the Opt-Out
The week's most consequential thread opened on Saturday afternoon when a data protection and clinical safety officer flagged Sections 260 and 261 of the new NHS Bill, which allow the Secretary of State to share data and override the national opt-out as they see fit. The accompanying observation was characteristically dry: "Lovely."
Within minutes the implications were being unpacked across the group. One GP partner with a long-standing interest in data ethics drew attention to Paragraph 47, which permits regulations stating that the processing of information "does not breach any obligation of confidence owed by the person processing the information." The room for non-direct-care expansion, with no mention of opt-outs, was noted with concern.
Another member observed that the bill goes "deep into FDP integration for all of health data as the Single Palantir Record," extending the architecture to private providers writing into the same record. The shared care implications were raised quickly afterwards: "And that's the shared care issue again of private providers dumping unprofitable work on general practice."
The thread ran into Tuesday, where the group connected it to the leaked NHS workforce plan and to the Met Police's separately blocked Palantir deal in London. By Wednesday the conversation had matured into a broader argument about whether the public are being asked to trust mechanisms that have already been engineered to bypass their stated preferences. The bill is not yet law, but the group's read is that the architecture is being built either way.
2. Securing Excellence, CIS2, and the Quiet Revolt of GP IT
Sunday afternoon a member asked, in apparent innocence, whether one could simply buy any laptop and run EMIS on it. The answer, predictably, ran for the next forty-eight hours. NHSE's updated Securing Excellence for Primary Care GP Digital Services, released on 8 May, became the reference document, and the group dissected its implications with the experience that only several decades of cumulative IT frustration can produce.
A GP educator pointed out that the new guidance includes the line "ICBs must support the practice's choice of accredited foundation solution," which a Welsh-influenced contributor immediately translated: "Guidance should have said, ICBs must prevent from using any alternative foundation solution. They often do the opposite, so that would have worked in practices favour."
The thread surfaced an uncomfortable revelation. An innovation-focused GP at a practice that has moved to Medicus reported that before they switched, "about 1000 staff at local hospital could read EMIS practices' notes without smart cards" and that the issue, as far as they were aware, had never been resolved. The group's moderator described it, tongue firmly in cheek, as "a failure of RBAC."
By Monday morning the conversation had moved to CIS2, the planned successor to physical smartcards. An NHS digital architect offered a measured view: CIS2 supports virtual identity, Windows Hello, and authenticator apps, but the rollout is being held back by hardware blockers and patchy WiFi at sites where staff need to log in. One GP shared that their practice had been forced to switch off two-factor authentication entirely after Microsoft Authenticator traffic refused to pass through the GovWifi network and there was no mobile signal to fall back on.
A senior IT operations contributor crystallised the principle at stake: "Role based PLUS solid authentication is the gold standard. But role based has an admin element in RA teams that I think the NHS wants to stop paying for." Authentication, like so much else, is being asked to do more with less.
3. Class I, Triage, and the Catastrophic Gaps in Tech Regulation Plans
Monday brought the HSJ scoop on what the paper called "catastrophic gaps in tech regulation plans," shared without comment by a clinical safety specialist with the prompt "Anyone going to own up!?" The MHRA's draft regulations had in fact been published the previous week, and an experienced safety specialist confirmed that the consultation closes on 19 June. The group was urged to respond.
The substantive concern centred on triage. AI receptionists, the safety specialist argued, decide whether to trigger a 999 message, whether to hand back to a human, whether to book an appointment and with whom and when. "All of that is triage." A data protection officer was crisp in agreement: "Is it making a decision on patient care for patients with urgent care needs? If so, it must be at least IIa, if not IIb. And I'm not sure I'll ever agree with Class I for that." And, with characteristic punch: "I just can't see it as ever acceptable that you can mark your own homework for something like triage."
A regulatory specialist with international perspective added a useful corrective. The proposed UK rules might allow Class I for some of these devices, but "that won't fly in the EU. So regardless, if you have any designs for the EU market, you're going to go down the NB/AB submission route anyway." The hot take from the group's moderator: "Maybe they'll start policing Class I?"
The thread fed naturally into the week's other regulatory milestone. On Thursday a digital health specialist shared that Tandem Health (which powers Accurx Scribe) had become the first standalone AI scribe in Europe to achieve Class IIa MDR certification. A regulatory specialist confirmed the significance, and another contributor observed that the announcement would have "a bunch of sour faces in the other providers' offices today." For all the noise about regulatory paralysis, somebody had just walked through the door.
4. When AI Writes the Complaint Letter
A surprisingly contested thread opened Monday morning when the group's moderator asked, on the back of teaching the weekend before, whether members were seeing a rise in AI-augmented patient complaint letters and what kind of volume increase they were experiencing.
The answers diverged sharply. One GP educator reported that "all complaints in last 3 months are AI written, not even checked on what expected outcome it lists and often suggesting actions practiced in America," and recounted phoning a complainant who then admitted the AI had over-egged the demand. A practice manager and an innovation-focused GP both took a different view, finding the structure and clarity helpful: "We have to of course filter for it often being non region based but I am okay about it if it empowers patients to get across what they previously couldn't."
A GP and digital health strategist added that the Parliamentary and Health Service Ombudsman now publishes suggested AI prompts on its own website to help patients frame complaints; the Ombudsman's helpful contribution being, perhaps, an unmistakable sign of where we are. One GP partner had received a complaint with "quotes of non existent legal citations," which felt like a particularly modern form of harm. Another offered the closing observation: "Tbh I'm more often saying 'I wish they'd used AI' rather than 'I wish they hadn't'. The worst ones are the ones where they ramble vaguely without their point being clear and use 3 pages to say something that could be said in a paragraph."
5. The Workforce Plan, the GDP Question, and a Genuinely Ambitious Argument
Wednesday was dominated by a leaked NHS workforce plan, surfaced via Doctors.net.uk, suggesting the NHS will recruit fewer staff overall and rely more on artificial intelligence. The plan apparently includes 49,000 more GPs by 2035, which a thoughtful contributor noted "sounds like the shift from hospital to community actually happening." The former head of the Institute for Fiscal Studies offered a "big oof" in the press, archived and shared by the same member.
The morning thread that followed ranged across NHS spending as a share of GDP (UK at 8.something percent, well below the EU average of around 10%, against the US at 16.6%), the hospital trolley problem in primary care referrals, and a sustained example by a data protection officer of how silently rejecting GP referrals does not make patients better; it makes them their GP's problem. Their borough's GPs, they noted, are seeing 60% more patients per GP than in 2019 yet subjective patient access is worse.
A same-day access GP brought the argument home: "It's not always about how much we spend, it's about where we spend it. More more is spent upstream on reactive healthcare when someone has become unwell rather than downstream on preventation. The NHS total outpatient follow-up spend is more than..." The morning closed with a wry observation from the group: "This morning's discussions may have helped re-radicalise many folk on the state of the nation."
That re-radicalisation set the tone for a remarkable late-evening thread which began with a simple question from a GP and digital health strategist: "How many lives are saved because of AI (or rather lost because AI was not used!) Hypothetically speaking, if 100 adverse outcomes are saved by AI but one additional adverse event happens, is that acceptable?" Over the next two hours, the group worked through statins, beta-blockers, unlicensed medication, drug licensing analogues, the Semmelweiss precedent, informed consent for AI-mediated decisions, and the rate at which AI capability is doubling.
The group's moderator captured one of the week's most quotable observations: "I can't help but think that AI is a modern Semmelweiss moment and we'll look back in 5 years and wonder why we put up such resistances." The immediate counterpoint, in the same breath: "Or... we'll be living in a mud hut by the banks of a dried out river Thames eating frogs." A public health data researcher tempered the moment with a pertinent qualifier: "I don't think we are really describing resistance here; we are more sceptical about whether the things we need will be built."

6. Conscientious Objection and the New Role at the Interface
Tuesday saw a discussion the group's moderator had not anticipated, after attending the NHS InSites Hi-Lites event on AVT and AI deployment. The presenters had described "active obstruction from some folk (over and above non-AI deployments)" within trusts. The group worked the implications gently and seriously. Is conscientious objection to AI a legitimate professional stance? What are the personal and population costs of becoming a conscientious objector to a technology that is doubling in capability every few months?
A data protection officer with environmental sensibilities was candid: "Using AI now for trivial tasks is environmentally atrocious, a real using a diesel SUV to do a 100m run to the shops then idling the engine while you're in there. Until that changes and we have UK-sovereign compute on UK-clean energy, I'm a conscientious objector to many use cases." Others made the workforce argument: AI tooling that erases junior grades undermines the training pipeline that sustains the consultant body, and that's a defensible reason to resist.
The group's moderator predicted, perhaps tongue not entirely in cheek, "the rise of a role that specifically manages that interface." Whatever you make of that prediction, the underlying point landed: the most progressive board on earth can be neutralised by a workforce that does not want to come along.
😄 Lighter Moments
The Sapient Intelligence release of HRM-Text, a hierarchical reasoning model with only one billion parameters, sparked a brief but joyous thread on what to call the new generation of compact, specialised models. The group's moderator settled it definitively with "small large language models," which a humour-tuned contributor immediately rebranded as "smöl models." The final word came from a regulatory specialist: "Smol model goes bbrrrr."
A GP educator's recurring complaint that Microsoft Authenticator could no longer back up to the cloud generated an image that captured perfectly the texture of NHS IT in 2026. The reply suggested using "a 2002 Toshiba laptop hanging around if anyone needs an upgrade from a CSU issued one."
Wednesday's facial recognition thread produced a particularly memorable observation from a same-day access GP whose ethnically ambiguous face has reportedly been identified by various biometric systems as "South Asian to Ethiopian/Eritrean to someone from the Caribbean." The same contributor's gloss on the technology: "We take your privacy seriously so will, record & surveil your images and store them forever."
The week also revealed that a contributor with a striking resemblance to the Prime Minister is regularly stopped in public. When asked what his father did, the answer was perfect: "He's not a Tool maker but he was a Screw," followed by the revelation that his mother used to send him out to talk to the prison inmates doing the family garden so she could have some peace. "I guess now she'd use ChatGPT!"
💬 Quote Wall
"I just can't see it as ever acceptable that you can mark your own homework for something like triage." – Data protection and clinical safety officer
"How can we be careful but not too careful? I leave that one to far wiser heads than myself." – GP and digital health strategist
"I can't help but think that AI is a modern Semmelweiss moment and we'll look back in 5 years and wonder why we put up such resistances." – Group moderator
"Or... we'll be living in a mud hut by the banks of a dried out river Thames eating frogs." – Group moderator, immediately afterwards
"It's not always about how much we spend, it's about where we spend it." – Same-day access GP
"We need better informed policy makers not those chasing clout." – Clinically-vexed GP
"We take your privacy seriously so will, record & surveil your images and store them forever." – Same-day access GP
"Smol model goes bbrrrr." – Regulatory specialist
"I think conscientious objection is the best case scenario if this continues. UK seems to be better than US right now." – Clinical AI engineer
"Today's is delayed, as Claude was helping me teach." – Group moderator, on the newsletter delay
📎 Journal Watch
Academic Papers & Key Studies
📎 The Use of AI in UK Healthcare – Policy Institute at King's College London The headline finding shared in group: 1 in 12 respondents said they have personally experienced a GP using an AI chatbot during a consultation. The full report covers public and clinician attitudes, with majority support for informed consent and opt-out across all scenarios. Read more
📎 LLM vs Human Neurologists - Diagnostic Comparison – medRxiv preprint, May 2026 Comparative study of LLM and human neurologists on diagnostic tasks. The most striking single number from the group's reading: 10% of LLM responses were rated as concerning, compared to 0% of human neurologist responses. Sparked a careful discussion about whether the human comparison cohort represented real-world working pressures. Read more
📎 Nature Digital Medicine paper shared on local AI in healthcare – Nature Digital Medicine Shared in the Saturday economics thread as evidence that local AI models can be both clinically and economically rational for healthcare systems. Read more
📎 An Artificial Intelligence Oracle for Proactive Population Health – Referenced by a public health researcher in the Wednesday ethics thread Cited as an example of "magical thinking" that nonetheless points to where AI's most defensible clinical contribution may lie: better coordination of care, real problem list curation, and management plans across settings.
Industry & News Articles
📎 Revealed: Catastrophic Gaps in Tech Regulation Plans – Health Service Journal, May 2026 Sharp critique of the MHRA's draft device regulations, particularly around classification of triage and decision-support tools. Triggered the group's regulatory deep dive and the call to respond to the consultation by 19 June. Read more
📎 Tandem's AI Scribe is now MDR Class IIa Certified – Tandem Health The first standalone AI scribe in Europe to achieve Class IIa MDR certification. Powers Accurx Scribe. A landmark for the sector and a rebuke to the line that the regulatory hurdle is impassable. Read more
📎 Sadiq Khan Blocks £50m Met Police Deal with Palantir – LBC News, May 2026 The London Mayor has blocked the Metropolitan Police's proposed £50m contract with Palantir. Shared in parallel with the wider Palantir-NHS conversation. Read more
📎 Pope Leo XIV's First Encyclical to Address AI – The Guardian, 18 May 2026 Magnifica Humanitas, the new Pope's first encyclical, will address the protection of human dignity in the age of artificial intelligence. A co-founder of Anthropic is among those joining the presentation. Read more
📎 AI Firm Sues Government Over Procurement Decision – Health Service Journal, May 2026 Another procurement dispute, shared with the resigned observation that there have been "quite a lot of alleged filings in the last year or so." Read more
📎 Anthropic Posts $559m Operating Profit in Q1 – LinkedIn analysis, May 2026 Anthropic now spends 56c per dollar of customer revenue on compute, down from 71c, and posted $559m operating profit for Q1. Numbers the group will want to keep front of mind during pricing and procurement conversations. Read more
Technical Resources & Guidelines
📎 Sapient Intelligence HRM-Text – GitHub New hierarchical reasoning model architecture from Sapient Intelligence; only 1B parameters, training method open-sourced. The model that prompted the "smöl" taxonomy debate. Read more
📎 NHSE: Securing Excellence in Primary Care GP Digital Services – NHS England, released 8 May 2026 Updated requirements for primary care GP IT including tightened cybersecurity. The reference document for the Sunday-Monday thread on what hardware and software practices may and may not use. Read more
📎 CIS2 Authentication – NHS Digital The Care Identity Service 2 platform, supporting modern authentication including virtual identity and Windows Hello. Reference shared as the planned successor to physical smartcards. Read more
📎 Black Pear, Hero Health, 6B Digital (Leeds), and Redrover Health EPR integration middleware suppliers shared in response to a Monday afternoon question about alternatives to IM1 / direct API integration. All retain dependencies on NHS England assurance, but offer practical entry points for products seeking record-level integration.
📎 Life Expectancy and Deprivation - Interactive – Public health researcher, GitHub Pages Interactive visualisation of life expectancy and causes of death by deprivation decile in England. Shared in the Saturday economics thread to anchor the "20 year HLE gap" argument in primary data. Read more
Policy Documents & Official Reports
📎 NHS Bill (HC Bill 9) - Sections 260 & 261 on Data Sharing – UK Parliament The new NHS Bill includes provisions allowing the Secretary of State to share data and override the national opt-out as they see fit, with Paragraph 47 protecting processors from breach-of-confidence claims. The legislative source document for the Saturday-Tuesday data sharing thread. Read more
📎 Petition: National Cardiac Screening for Young People – UK Government petitions Petition flagging that 1 in 300 young people screened by Cardiac Risk in the Young (CRY) have a hidden potentially life-threatening condition. Shared on Tuesday and triggered a measured screening debate about who would do the work and at what opportunity cost. Read more
📎 UK NSC Position on Sudden Cardiac Death Screening – UK National Screening Committee The current UK NSC position, due for review. Shared as the reference point against which the petition's claims should be assessed. Read more
📎 HSJ Digital Awards 2026 Shortlist – Health Service Journal The week closed with the news that a long-time group contributor has been highly recommended for Digital Innovator of the Year. Congratulations from across the group followed. Read more
🔭 Looking Ahead
The MHRA draft device regulations consultation closes on 19 June and the group has been urged to respond. Pope Leo XIV's encyclical Magnifica Humanitas is due for publication on Monday and is expected to set a moral frame for AI deployment that healthcare leaders may well be cited at over the coming year. The Medicus Open Day at Wilmslow Health Centre runs on Saturday 24 May, with additional capacity confirmed. NHS Hack Day's next event is being planned, most likely in London; subscribers can register interest via the project site. And the group's moderator has floated the prospect of an AI in the NHS panel-style podcast, drawing on members to discuss the topics covered here, with appraisal-friendly journal club elements. Early signals are warmly positive.
🧬 Group Personality Snapshot
This week the group reached its 50th issue and the timing felt right. The Wednesday late-evening ethics thread was the kind of exchange that you simply do not get on Twitter or LinkedIn: a GP and digital health strategist asking a Hippocratic question, a clinical AI specialist invoking Semmelweis, a public health researcher refusing to let the conversation collapse into either hope or despair, and the whole exchange staying productive past 11pm on a Wednesday in May. The Saturday Bayes Business School afterparty showed the group's range, moving in an hour from Spanish health spa vouchers for elderly residents who avoided admissions to the death of Richard Lehman and a perfect tribute from a public health researcher: a journal review picked from his BMJ column at random, and inevitably still brilliant.
The group's character is hard to summarise, but Wednesday's "we'll be living in a mud hut by the banks of a dried out river Thames eating frogs" landed precisely because the same person had, in the previous breath, made a serious case for the modern Semmelweiss moment. Few discussion communities sustain both registers in the same paragraph. This one does.
A note of remembrance closes the section. The group recorded its condolences this week on the death of Richard Lehman, the BMJ journal reviewer whose weekly column made primary care research readable and whose subversive academic warmth shaped a generation of GPs. He will be missed.
APPENDIX A: Detailed Activity Analytics 📊
📬 Total Messages: 514 across 7 days
📈 Peak Day: Wednesday 20 May (133 messages)
🔥 Most Active Period: Weekday mornings (07:00-10:00)
💬 Average/Day: 73.4 messages
🏖️ Weekend Activity: 27.4% (141/514)
💼 Weekday Activity: 72.6% (373/514)
🧠 Quietest Day: Friday 22 May (21 messages)
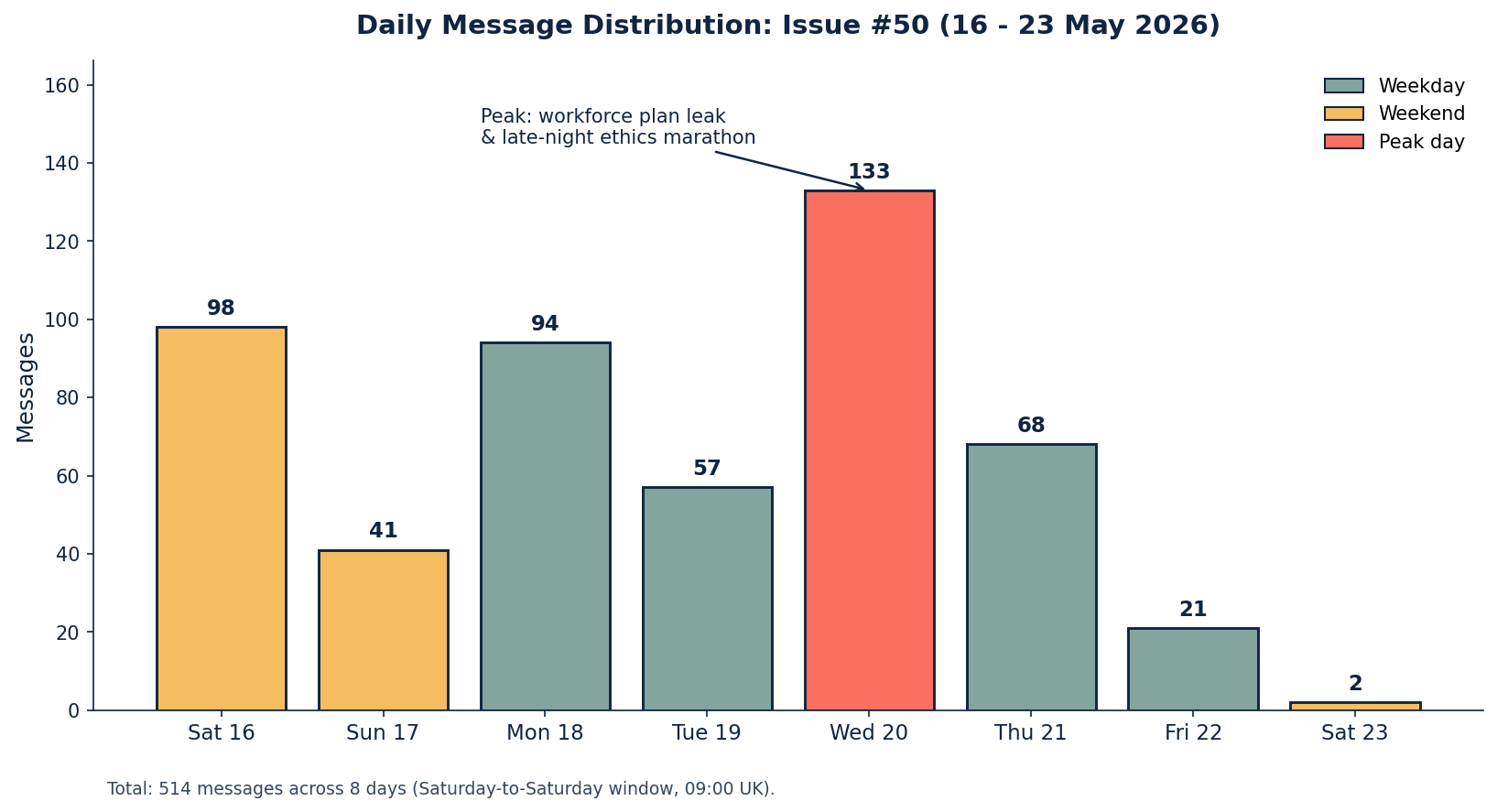
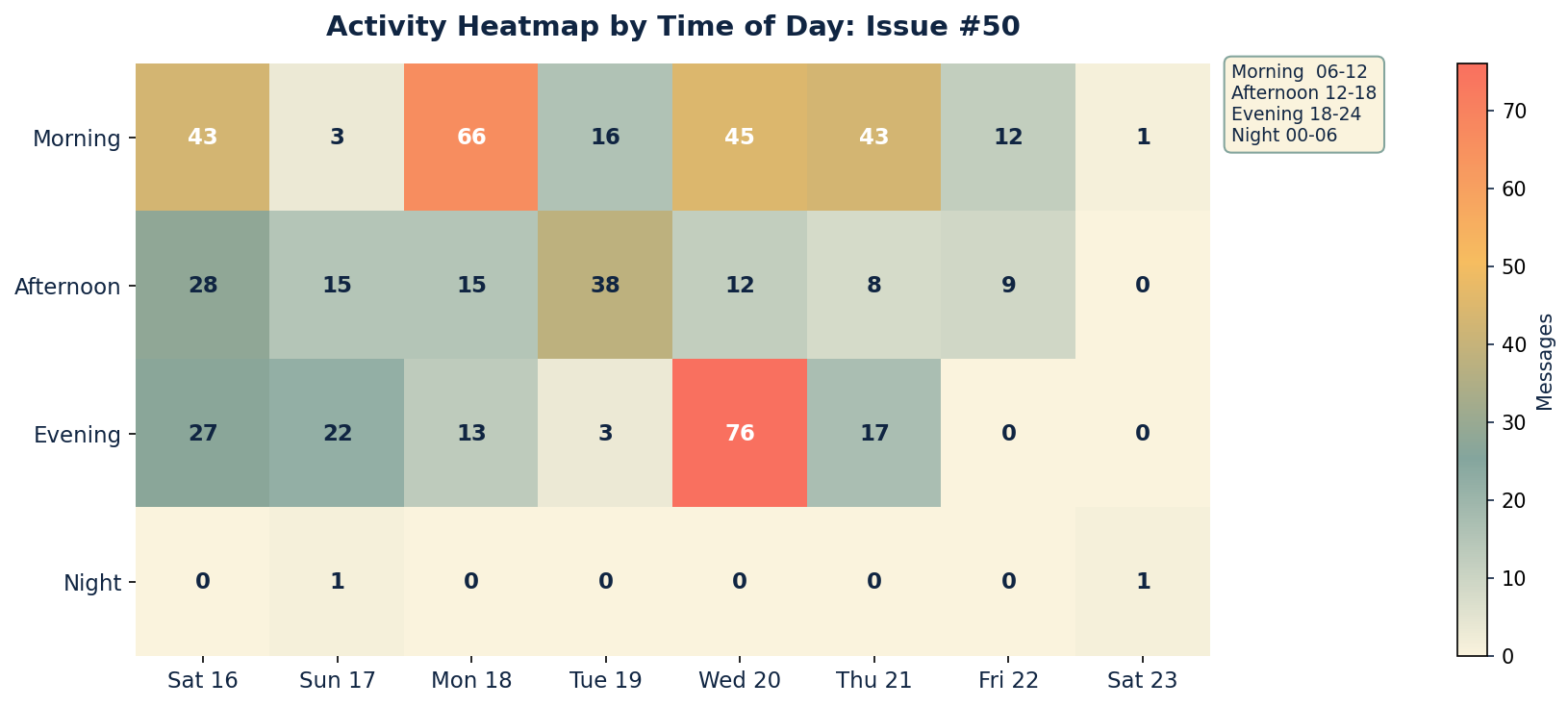
Insights: Wednesday's peak was driven by twin clusters: the morning workforce-plan-and-GDP discussion, and the late-evening ethics marathon that ran past 23:00. Saturday morning's continuation of the Bayes Business School conversation was the week's most sustained single-thread weekend session. Friday's drop to 21 messages broke a long-running pattern; possibly the cumulative cognitive load of the previous four days finally caught up with the room.
APPENDIX B: Enhanced Statistics
Top 10 Contributors (Role Descriptors Only)
1. Group Moderator (Digital Health & Clinical AI Specialist): 100 messages
2. Data Protection & Clinical Safety Officer: 47 messages
3. Clinical Safety Specialist: 37 messages
4. Clinically-Vexed GP: 33 messages
5. GP and Cardiology Liaison: 29 messages
6. Cardiology Consultant & Researcher: 23 messages
7. Public Health Data Researcher: 23 messages
8. Health Policy Researcher (Think Tank): 20 messages
9. GP and Digital Health Strategist: 16 messages
10. Practice Manager / Operations: 12 messages
Hottest Debate Topics
1. 🔥🔥🔥 Wednesday ethics marathon: hospital trolley problem, Semmelweiss analogue, AI device licensing (52 messages, single evening)
2. 🔥🔥🔥 NHS Bill Sections 260/261 and the Single Patient Record (38 messages across 4 days)
3. 🔥🔥🔥 GP IT, CIS2 authentication, and Securing Excellence (34 messages across 2 days)
4. 🔥🔥 MHRA draft regulations, triage classification and Class I gaming (28 messages across 2 days)
5. 🔥🔥 Workforce plan leak, NHS GDP comparisons, and referral rejection (26 messages, single morning)
6. 🔥🔥 Conscientious objection and active obstruction to AI deployment (22 messages across 2 days)
7. 🔥 AI-augmented patient complaint letters (18 messages, single morning)
8. 🔥 Bayes School longevity/prevention thread (16 messages, single afternoon)
Discussion Quality Metrics
• Evidence-Based vs Opinion Ratio: 36% of messages referenced papers, reports, primary documents, or tools
• Average Thread Depth: 6.4 messages per discussion thread (up from 5.1 in #44)
• Constructive Challenge Rate: 32% of responses offered alternative viewpoints or direct rebuttals
• External Resource Sharing: 41 unique links shared across the period
• Cross-Expertise Engagement: GPs, consultants, clinical safety officers, data protection specialists, public health researchers, regulatory specialists, AI engineers, practice managers, an academic theologian-adjacent thread, and at least one cardiologist with strong views on Tadalafil
Cross-Expertise Engagement
• At least 13 distinct professional backgrounds contributing this week
• Most cross-disciplinary thread: the Wednesday ethics marathon (GP, public health, clinical safety, data protection, digital health, regulatory, AI engineering)
• Notable knowledge transfer: a regulatory specialist clarifying EU MDR Class IIa pathway implications for UK products targeting EU markets
• 71% of major threads involved 3+ different professional perspectives
APPENDIX C: Daily Theme Summary
Saturday 16 May 2026
Primary Theme: NHS sustainability, prevention, and the new NHS Bill Key Discussion: The Bayes Business School conversation continued into the weekend, ranging across NHS GDP comparisons, prevention versus treatment economics, and the social determinants of healthy life expectancy. Mid-afternoon a data protection officer surfaced Sections 260 and 261 of the new NHS Bill on data sharing, which set up the week's constitutional thread. Secondary Discussions: Local AI models for sovereignty and economy; calorie restriction and longevity science; the German intelligence agency choosing a Palantir alternative. Notable: News of Richard Lehman's death broke late afternoon. The group's tribute was understated and warm.
Sunday 17 May 2026
Primary Theme: GP IT, hardware choice, and the move to Medicus Key Discussion: A direct question about running EMIS on personally-purchased hardware opened a two-day thread on the new NHSE Securing Excellence requirements (released 8 May), CSU restrictions, smartcard portability, and the practical reality of trying to use a Mac with the NHS smart card stack. Secondary Discussions: A LinkedIn post on clinical decision-making with incomplete information; the publication of newsletter #49; the Hard Fork podcast exchange as a calming counterweight to AI anxiety. Notable: Quietest substantive day of the week (41 messages), but the GP IT thread set the tone for a procurement-and-regulation Monday.
Monday 18 May 2026
Primary Theme: MHRA draft regulations, triage, and AI-augmented complaint letters Key Discussion: HSJ's "catastrophic gaps" article landed first thing and pulled the group into a forensic examination of the MHRA's draft proposals. The triage thread asked whether AI receptionists can ever defensibly be Class I and revealed unease about the gulf between proposed UK rules and EU MDR. In parallel, the group's moderator opened the AI-complaints thread, which produced sharply divided views. Secondary Discussions: CIS2 successor to physical smartcards; AVT context engineering; EPR integration middleware (Black Pear, Hero Health, 6B Digital, Redrover); Clippy 2.0 prompt injection humour. Notable: Monday produced the week's most consistent throughput at 94 messages and laid the regulatory foundations for Tuesday and Thursday.
Tuesday 19 May 2026
Primary Theme: NHS InSites Hi-Lites event, active obstruction, and the KCL report Key Discussion: The group's moderator reported live from the Hi-Lites event, including Cogstack and Alder Hey on-prem deployments. The references to active obstruction by trust staff sparked a measured discussion of conscientious objection. KCL's Policy Institute report The Use of AI in UK Healthcare landed mid-afternoon with the eye-catching finding that 1 in 12 respondents had personally experienced a GP using an AI chatbot. Secondary Discussions: Sapient Intelligence HRM-Text and "smöl" model taxonomy; sudden cardiac death screening petition and the UK NSC's position; BMA on AI risks; the IFS commentary on the leaked workforce plan. Notable: A relatively contained 57 messages, but the conversational ground was being prepared for Wednesday.
Wednesday 20 May 2026
Primary Theme: NHS workforce plan leak and the ethics of AI in clinical practice Key Discussion: The leaked NHS workforce plan dominated the morning, with the group working through GDP comparisons, hospital referral rejection economics, and a worked example contrasting an early referral pathway with the more common rejected-then-deteriorate pathway for a hip replacement. A medrxiv LLM-vs-neurologist preprint produced the eye-watering single number of 10% concerning responses (LLM) versus 0% (human). The evening produced one of the year's most ambitious ethics exchanges, running from a hypothetical to Semmelweiss to statins and beta-blockers to informed consent for AI use, all in two hours. Secondary Discussions: AI in transport hubs and facial recognition (Victoria, the Strand); the Kier Starmer doppelgänger thread; Bob Wachter's "A Giant Leap" book recommendation; OpenAI's discrete geometry conjecture result. Notable: Peak day at 133 messages, sustained across morning and evening. The single richest day in recent newsletters.
Thursday 21 May 2026
Primary Theme: Tandem/Accurx Class IIa, Pope Leo XIV, and the conscientious objection debate Key Discussion: The continuation of conscientious objection threads from Tuesday, with a GP partner's seatbelt analogy adding a much-shared frame. The MIT 95% no-ROI study was revisited and partially defended; the group's moderator argued the study was now "OLD on an AI timeline." The Tandem announcement of standalone Class IIa MDR certification was the most consequential single product news of the week. Sadiq Khan's blocking of the Met-Palantir deal landed mid-afternoon. The Pope Leo XIV encyclical with Anthropic involvement closed the day. Secondary Discussions: Eclipse pilot for prescribing safety and frailty (still early days); Anthropic Q1 $559m operating profit; a widely-cited analysis of Anthropic's compute cost ratio. Notable: 68 messages, the second-highest day, with significant external news in three different areas.
Friday 22 May 2026
Primary Theme: HR, whistleblowers, and an AI firm suing the government Key Discussion: A reflective Friday: the difficulty of removing consistently underperforming staff; the institutional incentives that target whistleblowers rather than the bullies they report; the latest in a series of procurement disputes brought to the High Court. Late afternoon saw the MyAutobot demo announcement, an AI agent for medical clinics that answers the phone, books appointments, and knows when the doctor is free. Secondary Discussions: Dark Star (1974) movie recommendation; Burdens of HSJ paywall and the universal blessing of burner email accounts. Notable: Quietest day at 21 messages.
Saturday 23 May 2026 (cutoff 09:00)
Primary Theme: HSJ Awards recognition Key Discussion: A long-standing group contributor was highly recommended for HSJ Digital Innovator of the Year. The thread of congratulations had only just begun by the 09:00 newsletter cutoff. Notable: 2 messages within the coverage window; a fitting upbeat note to end the week on.
AI in the NHS Weekly Newsletter is produced by Curistica Ltd for members of the AI in the NHS WhatsApp community. All contributors are anonymised. Views expressed are those of individual community members and do not represent any organisation.



