

Executive Summary
ReWIRED 2026 dominated the week, bringing the community together in person in Birmingham and sparking lively online exchanges about agentic AI, ambient voice technology governance, and the future of primary care systems. A passionate debate on AI liability and clinical responsibility ran across multiple days, crystallising around the question of who bears responsibility when AI tools get it wrong. The BMA GP Referendum closed with a resounding 99% No vote, and a national EMIS outage on Monday reminded everyone why system resilience and interoperability standards matter more than ever. The group also wrestled with the Federated Data Platform's future, debated whether Palantir's expanding UK footprint represents partnership or surveillance, and welcomed new members drawn in by the conference buzz.
Activity at a Glance
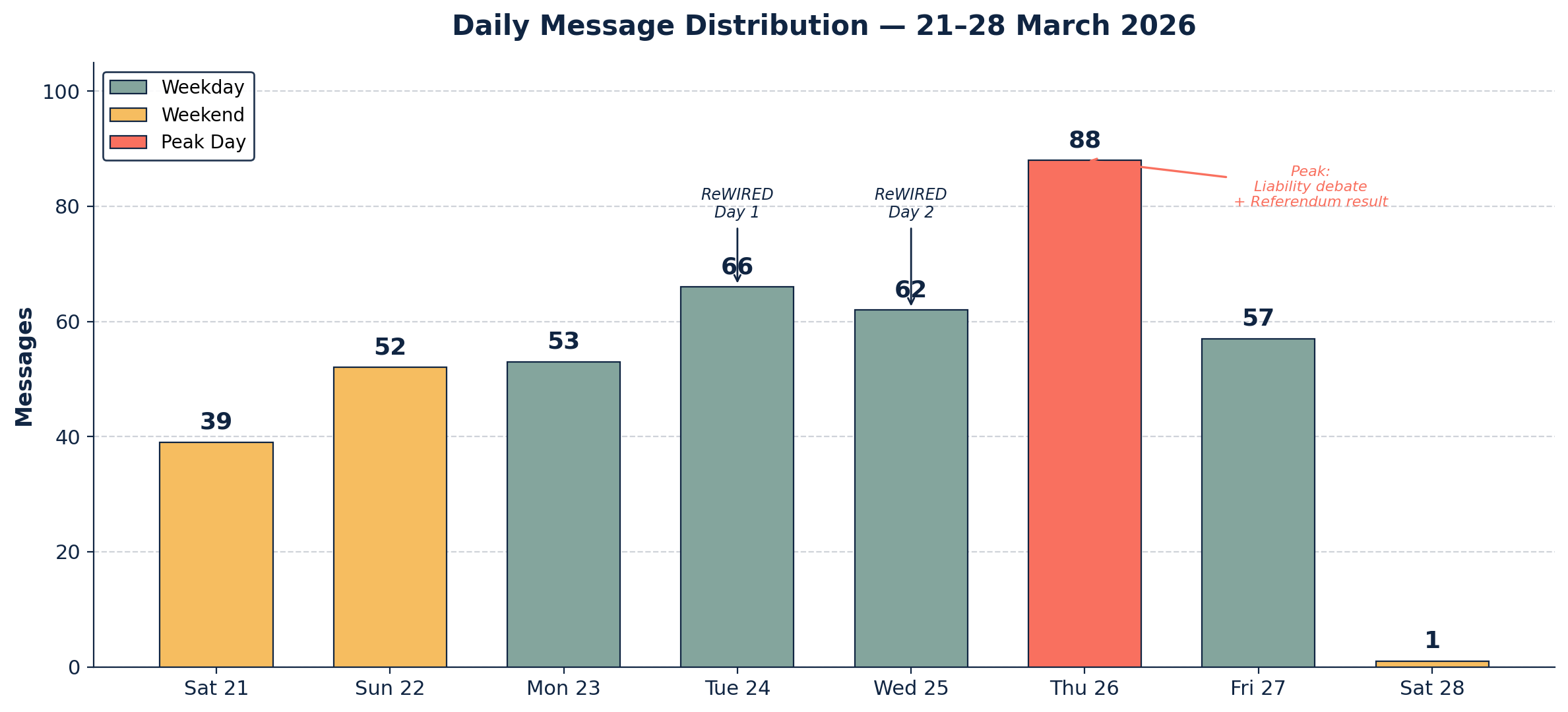
This week generated approximately 359 messages across 8 days, with peak activity on Thursday 26 March (88 messages) driven by the AI liability debate and the GP Referendum result. Morning hours (06:00–12:00) accounted for 43% of all traffic, and the top 10 contributors produced 48% of messages, with the remaining 52% distributed across more than 50 other participants — a healthy sign of broad engagement.
📌 Major Topic Sections
1. From Chats to Claws: Agentic AI Arrives in Healthcare
The week's centrepiece was a keynote delivered at a radiology conference on Friday 27 March, in which the group's moderator traced the evolution from chat-based AI through reasoning models to fully agentic systems that use tools, take actions, and work autonomously. The talk introduced the model-app-harness framework (developed by a prominent AI researcher at Wharton) — the idea that the same underlying model behaves very differently depending on how it is harnessed — and drew on real-world examples including Oxford's Trusted MDT cancer treatment planning system, already live in Q1 2026 with three specialist agents handling clinical summarisation, cancer staging, and treatment planning.
The talk also introduced the "lethal trifecta" — the point at which an agent combines access to private data, exposure to untrusted content, and the ability to take action. The community had already been discussing this risk earlier in the week. On Sunday 22 March, one member recommended Hermes Harness as an alternative to OpenClaw, while another urged running autonomous tools containerised in Docker, adding with characteristic candour:
"Don't ask me how I know." — A technically-minded GP
The keynote's provocative challenge to radiologists — "What if you just started building your solutions for the problems you face, and stopped waiting for other people to do it for you?" — resonated with a thread running throughout the week about vibe coding and democratised software development. On Tuesday, the moderator noted while attending ReWIRED that you could "vibecode OpenSAFELY work" while listening to a presentation, and on Wednesday the group debated the relative merits of Claude, ChatGPT, and Perplexity, with one member observing:
"I'm currently 9 hours into automating a job I do once a month that takes about 5 mins. WINNING!" — A technically-minded GP
The human costs of agentic working also surfaced. The moderator proposed the concept of a "MedMETR" — borrowing from METR's AI capability evaluation framework — to measure what length of human task chain an agent can reliably complete. He also wondered whether such frameworks could help manage brain fry and over-productivity in teams.
2. Who Bears Responsibility? The AI Liability Debate
Thursday 26 March saw the week's most sustained and substantive exchange, as the group grappled with the thorny question of liability when AI tools are used in clinical settings. The discussion drew contributions from GPs, clinical safety experts, digital health specialists, and health tech founders across more than 30 messages.
A GP with extensive digital health experience set out the core problem through a ventilator analogy:
"If the using clinician gets it wrong, that's their problem. If the hospital buys an inappropriate one through negligence, that's their problem. If the thing itself is faulty, that's the manufacturer's problem. Many AI suppliers want to pass the entirety of the last bullet to the clinician." — A digitally-experienced GP
The moderator pushed the conversation forward by arguing that real progress requires getting to a point where AI tools can sign off autonomously, with liability resting with the deploying organisation rather than the individual clinician. He cited Skin Analytics' DERM as a Class III device already structured this way and urged the group to think about starting with non-clinician deployment use cases.
A medical device regulation specialist noted that liability is context-dependent — if DERM is used by a non-clinician, liability sits with the manufacturer; if used by a clinician, it shifts to the clinician. This has yet to be tested in court.
The debate also touched on the limits of probabilistic systems in time-pressured consultations. The moderator challenged the group:
"If you are using it in a 10 minute consult, does anyone honestly believe that the end user will dig through the priors and posteriors before making a decision?" — Group moderator
One member referenced a well-known NHS case as a cautionary example of the NHS throwing clinicians under the bus to avoid institutional liability, while another noted that the concept of vendor-side insurance for AI errors — first discussed in the group several weeks ago with reference to ElevenLabs — remains unresolved, with insurers remaining "risk averse and charging a fortune."
A parallel thread on Friday explored similar territory from a different angle, with members debating whether clinicians should begin relinquishing control of notes to ambient voice technologies. One GP argued:
"If someone or something can reliably and safely do aspects of what I do better, then let's explore how to make it work." — An innovation-focused GP
Others pushed back, emphasising that clinical knowledge extends far beyond what is written in notes, and that current AVT outputs still contain hallucinations.
3. The Federated Data Platform: Partnership or Procurement Problem?
Sunday 22 March saw a lengthy and deeply engaged discussion about the NHS Federated Data Platform, prompted by articles about Palantir's expanding UK government contracts. The conversation drew on perspectives from BI specialists, data architects, health informaticians, and frontline GPs.
One member provocatively compared FDP to "a convenient wrapper to hide myriad failings of silo-centric EPR/PAS," arguing that as a parasitic BI approach, it is "only as good as the data they feed from." Another claimed that "a combination of Excel, SharePoint, and a pretty Power BI front end would be a whole pile better than FDP in my experience."
More constructive proposals emerged as the discussion deepened. A health data standards expert provided valuable historical context, tracing the origins of DICOM and HL7 back to mid-size suppliers and provider organisations that saw standards as a way to grow the market. He argued that NHS England has "defunded and disengaged from information standards activity" and called for the publication of FDP data models as a first step.
Several members proposed a component-driven, vendor-neutral approach rather than a single monolithic procurement, while others argued passionately that any data solution must be national, not regional, to deliver genuine population health benefits.
"What do we need to deliver better care, safer, faster and cheaper care to our patients?" — A health tech analyst
The Palantir dimension resurfaced repeatedly across the week. On Monday, a detailed summary of a major Observer investigation was shared, framing the relationship as a potential "Faustian pact." By Thursday, news emerged that NYC Health + Hospitals was ending its $4M Palantir contract, adding fuel to the sovereignty debate.
4. AVTs Under the Spotlight and the BMA Referendum
The week saw ambient voice technology come under increasing regulatory and community scrutiny. On Tuesday, NHS England published guidance on using AI-enabled ambient scribing products, prompting one clinical safety expert to express frustration:
"I'm just miffed why AVTs seem to be getting this level of treatment. Plenty of other, arguably higher risk technologies not getting the same treatment." — A clinical safety expert
A member with regulatory insight observed that "AVT techs are rapidly getting large footprint and we aren't always seeing the same embrace of regs and good practice that characterised other SaMD categories in recent years." Meanwhile, an AVT adoption/abandonment survey — a collaboration with a prominent regulatory academic — was circulated on Friday.
Running in parallel, the BMA GP Referendum dominated Wednesday and Thursday. The final push for votes on Wednesday morning ("14 minutes left!") gave way to the result on Thursday afternoon: a resounding 99% No vote. The group debated what this means in practice, with one member noting that "it's a recurrent theme in recent years that everyone says no and it gets enforced anyway," while another observed the difficulty of collective action when GPs are self-employed and cannot strike.
5. ReWIRED 2026: The Community Convenes
Digital Health ReWIRED (24–25 March, Birmingham) served as both a catalyst for in-person connections and a rich source of online commentary. The moderator chaired an AI panel on Tuesday afternoon and reported "LOADS" of questions from the audience afterwards. Images from the conference floor showed standing-room-only sessions and networking encounters between group members meeting for the first time.
The event also drew new members to the group, including a London-based GP who introduced himself as having "a keen interest in the effective enablers within primary care." Conference highlights shared by members included discussion of the AIDF (AI Deployment Framework) output and next steps, an overview slide on AI in radiology presented at the British Institute of Radiology, and news that the NHS App is set to become a "companion" over the next few years.
😄 Lighter Moments
The week's nostalgia award goes to the moderator, who — while preparing for ReWIRED — revealed that in the 1990s he was used by friends as a mobile "meet and greet" point on the dancefloor, even being made to wear a specific coloured hat. "I'm 6'5" and probably easy to spot," he noted. This prompted one member to conjure an image of him "in a Kangol blowing his whistle and raving out to The Time Frequency, Scotland's finest contribution to techno." The moderator confirmed his haunt was a club in Edinburgh, "mostly taps aff."
Wednesday delivered a gem when a member shared their automating-a-5-minute-job saga, prompting the reply: "Have you considered a job in management consultancy? You too can bill 9 hours for 5 minutes of real work."
One member described Google Meet as "the Happy Shopper of videoconferencing," while another, reflecting on the WhatsApp group's sheer volume, observed: "On this group, I pity people not glued to their WhatsApp at peak times as the volume of messages is something else."
And in possibly the week's most relatable moment, a member reported that they "broke Claude" while planning a trip to Switzerland, hitting usage limits just asking about holiday activities.
💬 Quote Wall
"The capability is really extraordinary, but the risk without governance is probably worse." — Group moderator (conference keynote)
"Many AI suppliers want to pass the entirety of the last bullet to the clinician, and the providers are often happy to hide behind clinical indemnity while signing the contract that says that." — A digitally-experienced GP
"Building software is no longer the bottleneck. All it is, is your ability to describe well what the problem is." — Group moderator (conference keynote)
"Our problem is not the tech delivery partner, it is the inability to finish what we start." — A healthcare informatician
"Governance isn't the enemy here. Nor is it about cutting down governance to allow for innovation. It's about innovating within that space." — Group moderator (conference keynote)
"If the notes start being massively lengthy because of AVT, then maybe impossible to pay attention — but I still come across hallucinations of all sorts." — A GP exploring AI tools
"Painting a rosy picture discourages change in the NHS." — A community health innovator
📎 Journal Watch
Academic Papers & Key Studies
- 📎 Health Systems Govern Only the Tip of the AI Iceberg — NEJM AI Over two thirds of physicians now use AI daily, mostly outside institutional oversight. The authors argue that governance designed for narrow AI tools fails for general-purpose platforms, and that lack of institutional engagement with consumer AI actually worsens risk. Read the paper (Shared 26 March)
Industry & News Articles
- 📎 How Tech Giant Palantir Was Recruited by the Police, NHS and Military — The Observer Deep investigative feature examining Palantir's expanding UK footprint across policing, health, and defence. Frames the relationship as a "Faustian pact" — powerful efficiency gains weighed against sovereignty and privacy risks. Read the article (Shared 23 March)
- 📎 NYC Health + Hospitals to End $4M Palantir Contract — Becker's Hospital Review Significant decision from across the Atlantic, adding evidence to the debate about Palantir's value proposition in healthcare. Read the article (Shared 26 March)
- 📎 Palantir UK Financial Data Contracts — LBC Health, Home Office, Finance — the broadening scope of Palantir's UK government data access. Read the article (Shared 24 March)
- 📎 UK Palantir Contracts — The Register Could the NHS scrap its Palantir contract and adopt systems built in Manchester or other regions? Read the article (Shared 22 March)
- 📎 AI Chatbot Users' Lives Wrecked by Delusion — The Guardian Cautionary feature on the real-world harms of consumer AI chatbot dependency. Read the article (Shared 26 March)
- 📎 Anthropic Says Testing "Mythos" Powerful New AI Model After Data Leak — Fortune A "step change in capabilities" leaked before official announcement. Read the article (Shared 27 March)
- 📎 Cybersecurity Stocks Plunge After Anthropic Claude Developments — Yahoo Finance Market implications of advancing AI capabilities in cybersecurity. Read the article (Shared 27 March)
- 📎 OpenAI Plans to Shut Down Sora Just 15 Months After Launch — Ars Technica Early signs of rationalisation in OpenAI's product portfolio. Read the article (Shared 24 March)
- 📎 Cohere Launches Open Source Voice Model for Transcription — TechCrunch A new entrant in the voice transcription space with an open-source model. Read the article (Shared 27 March)
- 📎 NHS App to Move from 'Front Door' to 'Companion' — Digital Health NHS England's vision for the NHS App's evolution over the next few years. Read the article (Shared 25 March)
Technical Resources & Guidelines
- 📎 Using AI-Enabled Ambient Scribing Products in Health and Care Settings — NHS England New guidance on AVT deployment requirements. Read the guidance (Shared 24 March)
- 📎 Agentic Engineering Patterns — simonwillison.net Comprehensive guide to agentic development patterns and best practices. Read the guide (Shared 22 March)
- 📎 LiteLLM PyPI Supply Chain Attack — FutureSearch / ox.security Critical warning: malicious PyPI versions of LiteLLM stealing cloud and crypto credentials. Read the alert | Read the analysis (Shared 25 March)
- 📎 Apple App Store Medical Device Declaration — Apple Developer Apple now requires intended use and safety warning declarations for medical device apps. Read the requirements (Shared 27 March)
- 📎 Declare Regulated Medical Device Status — Apple Pushed update requiring medical device questionnaire. A member noted: "Looks like intended use and safety warning now need to be provided for the listing." (Shared 27 March)
- 📎 Plaud Skills — Plaud.ai Plaud AI wearable getting skills/plugin capabilities. Read more (Shared 27 March)
- 📎 Gemini 3.1 Flash Live with Agents — Google AI Blog Google's Gemini voice model now live with agent capabilities. Read the blog (Shared 26 March)
Policy Documents & Official Reports
- 📎 Neighbourhood Health Framework and GPAD Changes — eGPlearning Key digital drivers in GP: GPAD appointment mapping changes and Neighbourhood Health Framework review. Watch GPAD changes | Watch framework guide (Shared 21 March)
- 📎 NHS FDP Explained: How Does It Work? — NHS England The canonical data model underpinning the FDP. Read the explainer (Shared 22 March)
🔭 Looking Ahead
The coming weeks look busy. Tech is Coming Home in Manchester on 15 April was flagged as an upcoming event to watch. The AVT adoption and abandonment survey — a collaboration with a leading regulatory academic — is still collecting responses, and results are eagerly awaited. The BMA GP Referendum's 99% No vote will now drive next steps from GPCEngland, with the group likely to see intense discussion of the implications. Apple's new medical device declaration requirements for App Store listings signal a quiet but potentially significant shift in platform-level governance. And the keynote's central challenge — build your solutions, build them safely, and embed governance from the first line of code — will no doubt continue to reverberate.
🧬 Group Personality Snapshot
This week captured the group at its most dynamic: a community that can pivot from a forensic debate about probabilistic liability in 10-minute consultations to fond memories of 90s rave culture in the space of an hour. The mixture of in-person ReWIRED encounters and rapid-fire WhatsApp exchanges created a particularly rich texture, with new members being welcomed warmly ("ReWIRED brings new folks!") and veterans continuing to challenge each other with the candour that defines this space. The group's ability to hold serious regulatory discussions alongside self-deprecating humour — "I broke Claude asking about Switzerland" — remains its signature quality. As one member put it, reflecting on the sheer volume: "I pity people not glued to their WhatsApp at peak times." At its best, this community models what professional discourse should look like: expert, engaged, irreverent, and unafraid to disagree.
APPENDIX A: Detailed Activity Analytics 📊
Metric Value 📬 Total Messages 359 📈 Peak Day Thursday 26 March (88 messages) 🔥 Most Active Period 08:00–12:00 💬 Average/Active Day 51.3 messages 🏖️ Weekend Activity 25.6% (92/359) 💼 Weekday Activity 74.4% (267/359)
Daily Message Distribution:
Activity Heatmap by Time of Day:
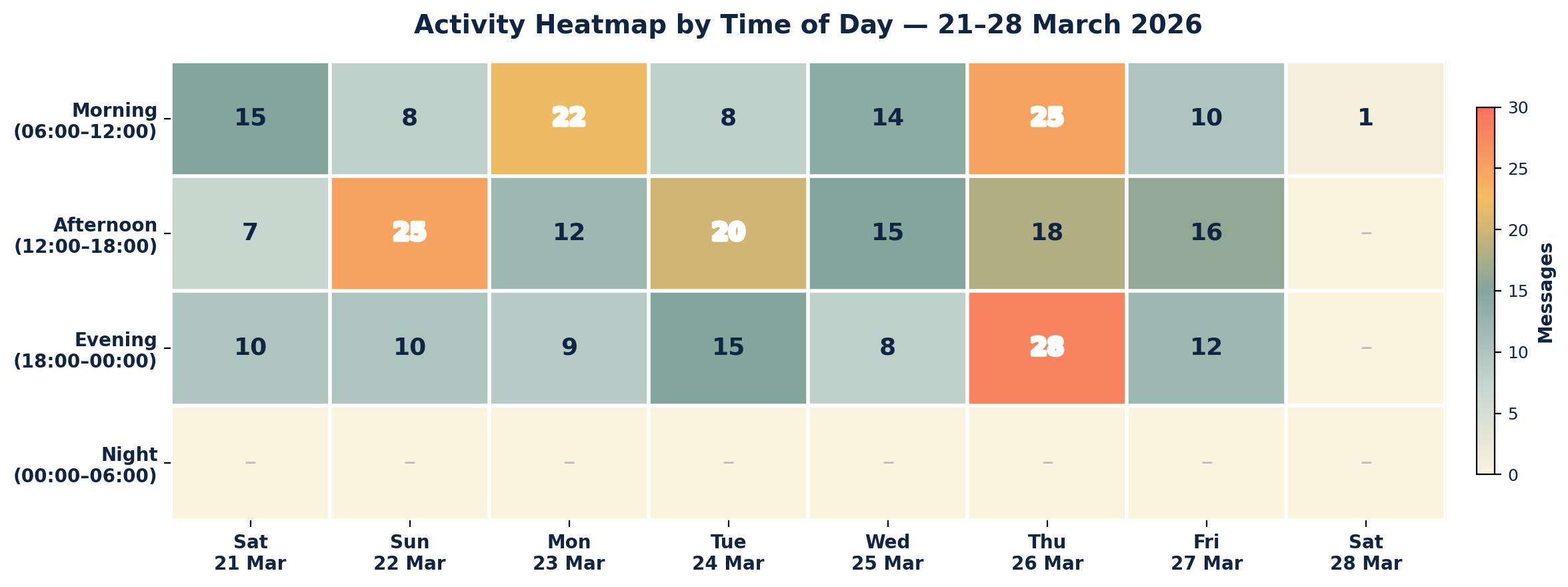
Key Insights: Thursday's spike was driven by the convergence of the AI liability debate, GP Referendum result, and conference preparations. Morning engagement (08:00–12:00) consistently dominated, suggesting professionals checking in before or between clinical sessions. Weekend activity remained substantial (25.6%), reflecting a community that engages beyond working hours.
APPENDIX B: Enhanced Statistics
Top 10 Contributors (Role Descriptors Only):
- Digital Health & Clinical AI Specialist (Group Moderator): 87 messages
- Innovation-Focused Health Tech Commentator: 23 messages
- Digitally-Experienced GP: 21 messages
- Clinical AI and Safety Specialist: 18 messages
- Health IT Architecture Analyst: 18 messages
- Health Tech Analyst: 16 messages
- Community Health Innovator: 13 messages
- Medical Device and AI Regulation Specialist: 11 messages
- Digital Health News Curator: 10 messages
- Clinical Informatician: 9 messages
Hottest Debate Topics:
- 🔥🔥🔥 AI liability, clinical responsibility, and vendor indemnity (30+ messages across 3 days)
- 🔥🔥🔥 NHS Federated Data Platform architecture and Palantir contracts (40+ messages across 4 days)
- 🔥🔥🔥 Agentic AI capabilities and governance (keynote + discussion, 25+ messages across 3 days)
- 🔥🔥 AVT regulation and clinical autonomy (20+ messages across 3 days)
- 🔥🔥 BMA GP Referendum and contract dispute (15+ messages across 3 days)
- 🔥🔥 AI tool preferences: Claude vs ChatGPT vs Perplexity (15+ messages on 1 day)
- 🔥 EMIS outage and system resilience (12+ messages on 1 day)
Discussion Quality Metrics:
- Evidence-Based vs Opinion Ratio: approximately 30% of messages referenced papers, guidelines, data, or external sources
- External Resource Sharing: 42+ unique links shared across the period
- Cross-Expertise Engagement: contributions from GPs, clinical safety officers, medical device specialists, health informaticians, BI analysts, data architects, regulatory specialists, and health tech founders
- Most Cross-Disciplinary Topic: AI liability debate (clinical, legal, regulatory, commercial, and ethical perspectives)
APPENDIX C: Daily Theme Summary
Saturday 21 March
Primary Theme: AI safety foundations — security, pen testing, and adversarial vulnerabilities Key Discussion: The group explored penetration testing standards (OWASP), the implications of OpenClaw making white-hat testing accessible to the masses, and the need for foundational AI safety/security training at undergraduate and postgraduate level. The moderator argued that whether tech is classified as a device or not, it can still have safety, privacy, and security issues. Secondary Discussions: DTAC effectiveness and tick-box compliance concerns; Newsletter #41 and podcast distribution; EHR integration risk research; GP Referendum voting reminder; Neighbourhood Health Framework and GPAD changes Notable: A clinical safety standards expert noted the standard "needs shoring up" significantly. Publication of Newsletter #41 and podcast updates.
Sunday 22 March
Primary Theme: NHS Federated Data Platform — architecture, procurement, and alternatives Key Discussion: A deeply engaged debate spanning 40+ messages about whether FDP delivers genuine value or merely wraps existing system failures. Members proposed component-driven, vendor-neutral approaches and called for publication of FDP data models. Historical context from DICOM and HL7 standards development was cited. Secondary Discussions: Agentic development tools (Hermes Harness, OpenClaw, NemoClaw); triage system enquiries; canonical data model progress; BI simulation for A&E scenarios Notable: Several members expressed interest in convening a roundtable to produce a position paper on NHS data architecture.
Monday 23 March
Primary Theme: EMIS national outage and system resilience Key Discussion: A national AWS-related outage affecting EMIS (and other systems) prompted discussion about primary care system stability, monopoly risks, and the need for competition. The moderator emphasised this "emphasises the importance of a more stable solution for primary care." Secondary Discussions: Palantir Observer investigation and UK sovereignty concerns; GP2GP bulk data transfer history; EPR switch service mandate proposal; information standards and interoperability; GP Autopilot/Dyad AI for coding letters; NAO AI assurance framework; Digital health solutions for A&E (Middle East tender) Notable: A health data standards expert provided rich historical context on GP2GP specifications from 25 years ago, noting the centre's reluctance to take liability for standardisation.
Tuesday 24 March
Primary Theme: ReWIRED Conference Day 1 — networking, panels, and AVT governance Key Discussion: The moderator chaired an AI panel at 16:30 and reported strong audience engagement. NHS England's new AVT guidance was shared, prompting debate about why ambient voice technologies are receiving disproportionate regulatory attention compared to other arguably higher-risk technologies. Secondary Discussions: Club culture nostalgia and 90s references; Palantir UK finance and surveillance state concerns; Sora shutdown; blockchain/NFT/FDP jokes; AVT publicity cycle compared to previous tech hype; AIDF output discussion Notable: New members began joining following ReWIRED encounters. Conference images showed standing-room-only sessions.
Wednesday 25 March
Primary Theme: AI tool stability and preferences — Claude vs ChatGPT vs Perplexity Key Discussion: A candid exchange about the relative stability, usability, and value of different AI platforms. Members shared experiences of crashes, rate limits, and workarounds, with one brave soul admitting "6 days of Claude and I don't see the hype" to a notoriously Claude-loving group. Secondary Discussions: BMA GP Referendum final voting push (closing at noon); LiteLLM supply chain security attack warning; ReWIRED Day 2 networking; new member welcomes; 9-hours-automating-5-minutes-of-work; Microsoft Teams frustrations; NHS App companion evolution Notable: The GP Referendum closed at noon with over 15,000 votes cast (49.38% turnout). A member was sitting OSCE exams in Birmingham while the conference ran nearby.
Thursday 26 March
Primary Theme: AI liability, clinical responsibility, and governance frameworks Key Discussion: The week's most substantive debate — over 30 messages exploring who bears responsibility when AI clinical tools get it wrong. Covered ventilator liability analogies, Skin Analytics Class III regulatory pathway, deterministic vs probabilistic system limitations, vendor-side insurance, and the case for starting with non-clinician deployment. Referenced a landmark NHS liability case and the NEJM AI "iceberg" governance paper. Secondary Discussions: BMA GP Referendum result (99% No); Gemini voice model with agents; Palantir NYC contract ending; conference keynote preparations ("From Chats to Claws"); Guardian article on AI chatbot harms; Apple medical device questionnaire; GMC and race-related regulatory concerns Notable: The moderator shared the NEJM AI paper "Health Systems Govern Only the Tip of the AI Iceberg" — directly relevant to the liability discussion. Conference keynote title revealed: "From Chats to Claws."
Friday 27 March
Primary Theme: Conference keynote — agentic AI in healthcare and the model-app-harness framework Key Discussion: The moderator delivered and shared a detailed keynote summary covering the evolution from chat-based to agentic AI, the model-app-harness framework, Oxford's Trusted MDT system, OpenClaw's lethal trifecta, vibe coding democratisation, and the central message that "the harness matters as much as the model." Secondary Discussions: AVT adoption/abandonment survey; Apple App Store medical device requirements; MedMETR proposal for agent reliability; EMIS-X assurance timeline; Anthropic Mythos model leak; Cohere voice model launch; care home feedback system interest; clinical note hallucinations vs AVT trust; Plaud AI getting skills Notable: The keynote's challenge to radiologists to start building their own solutions rather than waiting for vendors encapsulated the week's overarching theme.
Saturday 28 March
Primary Theme: NHS change and innovation culture Key Discussion: A single early-morning message urging the community to capture the full picture of effort invested versus success gained, arguing that "painting a rosy picture discourages change in the NHS." Notable: A reflective note to close the week's intense discussions.
AI in the NHS Weekly Newsletter is produced by Curistica Ltd for members of the AI in the NHS WhatsApp community. All contributors are anonymised. Views expressed are those of individual community members and do not represent any organisation.



